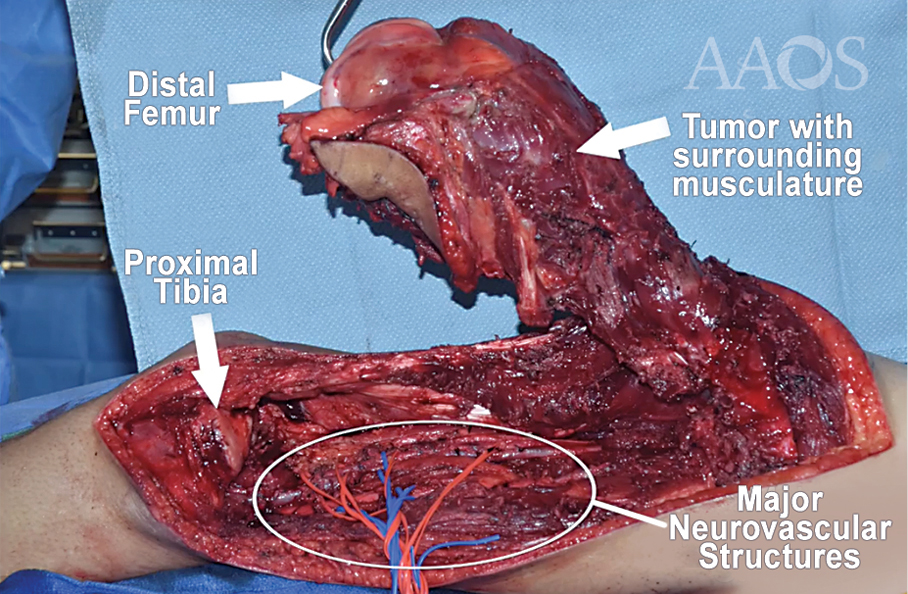
Fig. 1 In this AAOS Orthopaedic Video Theater video, Joseph Dominic Giacalone et al demonstrate parosteal osteosarcoma dissected from remaining soft tissues.
Published 11/25/2024
|
Michael DeRogatis, MD, MS; Paul S. Issack, MD, PhD, FAAOS, FACS
Editor’s note: The following article is a review of a video available via the AAOS Orthopaedic Video Theater (OVT). AAOS Now routinely reviews OVT Plus videos, which are vetted by topic experts and offer CME. For more information, visit aaos.org/OVT.
Osteosarcoma is the most common primary bone cancer in children and adolescents. It is a malignant lesion, and common extremity sites include the distal femur, proximal tibia, and proximal humerus. Radiologic metastases can be identified at diagnosis 25 percent of the time, with the lungs being the most common site. Treatment of distal femoral osteosarcoma involves the use of neoadjuvant chemotherapy, followed by limb-salvage surgery. Adjuvant chemotherapy is restarted after surgery.
The AAOS OVT video titled “Distal Femur Replacement from a High-Grade Chemoresistant Osteosarcoma” demonstrates a limb-sparing surgery involving distal femur replacement to treat a patient aged 16 years with knee pain and instability and a posterior bone lesion on his left femur. Biopsy confirmed the lesion to be a high-grade parosteal osteosarcoma. After 3 months of preoperative chemotherapy, the tumor grew and metastasized, necessitating resection and distal femur replacement.
The authors chose a lateral approach to excise the biopsy tract with a wide margin. They developed a plane between the vastus lateralis and intermedius, leaving the biopsy site in continuity with the tumor. A plane with clear margins was developed, leaving the tumor intact. A 4 cm margin proximal to the most proximal extent of the intramedullary tumor component was identified as the resection point. The biceps femoris was released to give access to the neurovascular bundle. Doppler ultrasound was used to identify and free up the popliteal artery, which was adherent to the tumor. Geniculate vessels were ligated. After dissecting around the tumor with a wide margin, the surgeon released the knee ligaments. The distal femur was then transected with a 4 cm margin based on preoperative MRI. The vastus intermedius, vastus medius, and vastus lateralis were left on the resected femur enveloping the tumor. One centimeter of the proximal tibia was then resected and prepared for the tibial implant.
The femoral canal was then reamed, and a trial prosthesis was assembled. After the implant sizes were confirmed, the final prosthesis was assembled on the back table. Cement was injected in the femoral and tibial canals, followed by placement of the final implants. The knee demonstrated full extension and flexion without tension on the soft tissues. The wound was irrigated with sterile saline and diluted betadine. The biceps femoris was approximated to the vastus lateralis. Postoperative therapy and adjuvant chemotherapy were initiated.
Overall, this video is a detailed and technically excellent demonstration of the steps of osteosarcoma resection and distal femur replacement. It will be of high educational value to both novice and expert orthopaedic oncologists.
Michael DeRogatis, MD, MS, is an orthopaedic surgery resident at St. Luke's University Health Network in Bethlehem, Pennsylvania, and serves as a resident member of the AAOS Now Editorial Board.
Paul S. Issack, MD, PhD, FAAOS, FACS, is a clinical associate professor in the Department of Orthopaedic Surgery, Weill Cornell Medical College, and a trauma and adult reconstruction orthopaedic surgeon at New York–Presbyterian/Lower Manhattan Hospital. He is also a member of the AAOS Now Editorial Board.
Video details
Title: Distal Femur Replacement from a High-Grade Chemoresistant Osteosarcoma
Authors: Joseph Dominic Giacalone; Julia Alexandra Matalon; Robert McCunney, MD; James C. Wittig, MD, FAAOS; and Kaitlin Zeedyk, PA-C
Published: January 31, 2024
Time: 10:58
CME: 0.75 credits
Tags: Distal Femur Replacement, Osteosarcoma, Ortho Oncology, CME
Visit aaos.org/OVT to view this award-winning title and more than 1,600 other videos from across orthopaedic topics, institutions, practice management, and industry.