
Fig. 1 Purely dynamic stabilization of syndesmosis
Courtesy of Annunziato Amendola, MD, FAAOS
Published 12/18/2024
|
Conor N. O’Neill, MD; Charles R. Reiter; Annunziato Amendola, MD, FAAOS
Ankle syndesmosis injury, often referred to as a high-ankle sprain, is common in athletics, comprising up to 20 percent of all ankle sprains. Indications for surgical fixation include acute injury with instability of the ankle.
The quality of surgical reduction is thought to be directly associated with functional outcomes. Surgical fixation methods have evolved over time, progressing from rigid screw fixation to anatomic repair with arthroscopy. Arthroscopy continues to play an important role in the diagnosis of syndesmotic injury, allowing surgeons to accurately diagnose dynamic instability and visualize reduction. This article provides a brief overview of the evolution of syndesmotic fixation and some insights into future directions.
Fig. 1 Purely dynamic stabilization of syndesmosis
Courtesy of Annunziato Amendola, MD, FAAOS
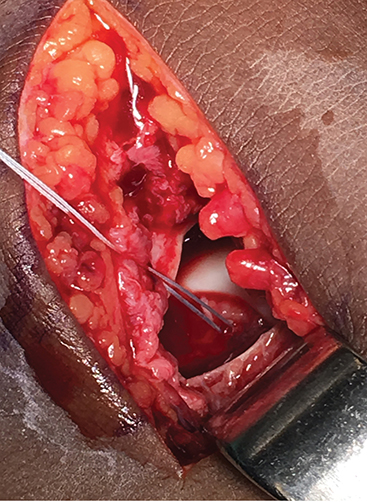
Fig. 2 Deltoid reconstruction
Courtesy of Annunziato Amendola, MD, FAAOS
Historically, the gold standard for surgical management of ankle syndesmosis injuries has been open reduction and screw fixation. This method involves placement of one or two cortical screws, with some surgeons opting to use a plate as well. The decision to utilize one versus two screws is based largely on surgeon preference; however, cadaveric studies have suggested biomechanical benefits of two-screw fixation over one-screw fixation. Although concomitant fracture pathology may affect surgical decision making, surgeons’ preferred fixation method typically remains consistent regardless of injury severity.
In 2010, a survey of orthopaedic surgeons conducted by Bava et al showed that 75 percent of respondents routinely used rigid fixation methods with 3.5 mm (51 percent) or 4.5 mm (24 percent) cortical screws. Of those surgeons, nearly half used a single screw, whereas the other half used two screws, and roughly two-thirds preferred four cortices to three cortices. This finding contrasts the results of an international survey of orthopaedic surgeons in 2021 that found that screw fixation alone was routinely performed by only 30 percent of respondents in favor of dynamic fixation or hybrid fixation methods.
The relative shift away from rigid screw fixation of the syndesmosis can be explained by the success of newer, dynamic fixation options, such as suture button (SB) fixation, and the drawbacks of screw fixation, notably the limitation of physiologic ankle motion and the common requirement of a second surgical procedure for hardware removal. Although there remains no consensus regarding screw removal, most surgeons routinely opt for removal within 3 to 6 months postoperatively. Despite this, there remains no definitive evidence to justify screw removal; thus, the second procedure may lead to undue costs and risks.
SB fixation
Dynamic stabilization with an SB device was developed to allow for physiologic micromotion of the ankle and to allow the fibula to settle within the tibial incisura (Fig. 1). Gardner et al reported a 52 percent incidence of malreduction of tibiofibular syndesmosis in Weber C ankle fractures treated with screw fixation. Studies have confirmed that dynamic fixation does, in fact, allow for micromotion, resulting in improved reduction and longer stability, which promote early mobility, weight bearing, and faster return to sport.
With the advent of dynamic stabilization of the syndesmosis, numerous studies have supported its use over traditional screw fixation. A large Canadian randomized clinical trial showed superiority of an SB technique over screw fixation, with better reduction, quicker return to work, and no need for routine hardware removal. A recent meta-analysis of randomized, controlled trials found that dynamic fixation led to a significantly reduced risk of complications compared with screws, in addition to significantly higher patient-reported outcomes.
Although many of these studies have focused on short-term outcomes and complications, such as early mobility and return to the OR, the long-term effects of anatomic syndesmotic reduction on the development of ankle arthritis remain in question. In a recent randomized, controlled trial comparing SB to screw fixation, the dynamic fixation group had improved American Orthopaedic Foot and Ankle Society scores and a lower incidence of ankle osteoarthritis at 5-year follow-up. The SB group also had a significantly smaller difference between the injured and uninjured contralateral anterior tibiofibular distance following fixation. The importance of anatomic reduction in the fixation of syndesmotic injuries has become clear over the years, leading to further development of anatomic reconstructions.
Technical pearls
- Ensuring anatomic reduction of the syndesmosis is essential for achieving favorable long-term results. This should be verified with either open or arthroscopic methods.
- The syndesmosis functions as a synovial joint, moving in three planes. Fixation should aim to minimize damage to the articular cartilage and interosseous ligament.
- The anterior inferior tibiofibular ligament (AITFL) plays a crucial role in resisting external rotation forces. AITFL repair, along with SB fixation, enhances stability against diastasis and external rotation.
Anatomic repair
The principle of anatomic repair is focused on the four main structures of the intact syndesmosis: AITFL, posterior inferior tibiofibular ligament (PITFL), intraosseous ligament, and inferior transverse ligament. A recent study by Lin et al compared screw fixation with direct anatomic AITFL repair, finding no differences in CT radiographic parameters but improved patient-reported outcome. Zhan et al showed that syndesmotic SB fixation paired with AITFL anatomic repair had equivalent reduction and functional outcomes but earlier rehabilitation and fewer complications compared with screw fixation. A biomechanical study by Shoji et al showed superiority of SB fixation with AITFL suture tape augmentation compared with SB alone and screw fixation. The combination of SB and AITFL augmentation most closely resembled the dynamic stability of the intact syndesmotic model. Schottel et al reported that anatomic repair using suture anchors for the deltoid ligament and PITFL was not inferior to screw fixation in external rotational stability in a cadaveric model (Fig. 2).
Role of arthroscopy
Arthroscopy allows for direct visualization of the syndesmosis, ensuring accurate reduction and fixation. Studies have shown that arthroscopic-assisted fixation can lead to better outcomes in terms of alignment and stability compared to traditional methods. Arthroscopy provides a clear view of the syndesmotic joint, allowing surgeons to make real-time adjustments and ensure proper alignment. Patients undergoing arthroscopic-assisted procedures often experience quicker rehabilitation and return to normal activities than those who undergo open surgery. The minimally invasive nature of arthroscopy reduces soft-tissue damage, contributing to faster healing and less postoperative discomfort. Additionally, the ability to address concomitant intra-articular injuries during the same procedure can enhance overall recovery and reduce the need for subsequent surgeries.
Rehabilitation
Rehabilitation after syndesmotic fixation depends on the severity of injury. Syndesmotic fixation associated with fracture or deltoid disruption is treated with touch weight bearing for 6 weeks regardless of screws or SB fixation. A CAM (controlled ankle motion) walker is used to allow for early range-of-motion therapy and reduce swelling after surgery. Weight bearing is begun after 6 weeks. The authors prefer removing the screws after 8 weeks to avoid screw breakage.
More subtle injuries without gross widening treated with SB fixation involve early weight bearing as tolerated and progression of weight-bearing therapy. With screw fixation, patients often need to avoid weight-bearing activities for a longer period, usually around 6 to 8 weeks, to ensure proper healing and to prevent screw breakage or loosening.
This method provides rigid stabilization but may require a second surgery to remove the screws before full weight bearing can commence. In contrast, SB fixation allows for earlier mobilization and weight bearing, often within a few weeks after surgery.
This dynamic fixation method maintains the necessary reduction while permitting some physiological movement, which can offer patients a faster recovery and return to normal activities.
Future directions
Given the focus on anatomic reduction and its potentially protective factors against the development of ankle arthritis, accurate diagnosis of both frank and subtle syndesmotic instability has become increasingly important. Historically, physical exam, radiographs, CT, and MRI have been used for diagnosis of syndesmotic injury, but the advent of weight-bearing CT (WBCT) scan has been beneficial for the detection of subtle instability. Further development of WBCT protocols may be beneficial in the diagnosis of subtle syndesmotic injury.
Cadaveric studies have shown that external rotation stress in addition to axial load is important for demonstrating syndesmotic widening. Development of platforms allowing for external rotation torque during WBCT may increase diagnostic yield in assessing subtle syndesmotic instability. Additionally, software measurement tools integrating multiple measurements into artificial intelligence algorithms may allow for more accuracy in identifying different patterns of abnormality and instability of the ankle syndesmosis.
Take-homes
The management of ankle syndesmosis injuries has significantly evolved, with a shift from traditional screw fixation to dynamic stabilization methods such as SB fixation.
This transition is driven by the need for better functional outcomes, fewer complications, and quicker recovery times. The importance of anatomic reduction, often aided by arthroscopy, cannot be overstated, as it is crucial for long-term joint health and stability.
Future advancements, particularly in diagnostic imaging and artificial intelligence–driven tools, promise to further enhance the precision and effectiveness of treatment. Ultimately, the focus remains on achieving optimal patient outcomes through innovative and evidence-based surgical techniques.
Conor N. O’Neill, MD, is a current sports medicine fellow and previous foot and ankle fellow at Duke University. He has a particular interest in the management of cartilage and ligamentous injuries and the role of limb alignment as it pertains to knee and ankle pathology.
Charles R. Reiter is a fourth-year medical student at Virginia Commonwealth University who is pursuing a career in orthopaedic surgery.
Annunziato Amendola, MD, FAAOS, is the AAOS first vice president. He serves as the Virginia Flowers Baker Distinguished Professor of Orthopaedic Surgery; chief of the Sports Medicine Division; executive director of the James R. Urbaniak, MD, Sports Sciences Institute; and head team physician and chief medical officer for Duke Athletics, all at Duke University.
References
- Gardner MJ, Demetrakopoulos D, Briggs SM, et al: Malreduction of the tibiofibular syndesmosis in ankle fractures. Foot Ankle Int 2006;27(10):788-92.
- Grassi A, Samuelsson K, D’Hooghe P, et al: Dynamic stabilization of syndesmosis injuries reduces complications and reoperations as compared with screw fixation: a meta-analysis of randomized controlled trials. Am J Sports Med 2020;48(4):1000-13.
- Thornes B, Shannon F, Guiney AM, et al: Suture-button syndesmosis fixation: accelerated rehabilitation and improved outcomes. Clin Orthop Relat Res 2005;(431):207-12.
- Cottom JM, Hyer CF, Philbin TM, et al: Transosseous fixation of the distal tibiofibular syndesmosis: comparison of an interosseous suture and endobutton to traditional screw fixation in 50 cases. J Foot Ankle Surg 2009;48(6):620-30.
- Sanders D, Schneider P, Taylor M, et al; Canadian Orthopaedic Trauma Society: improved reduction of the tibiofibular syndesmosis with tight rope compared with screw fixation: results of a randomized controlled study. J Orthop Trauma 2019;33(11):531-7.
- Ræder BW, Figved W, Madsen JE, et al: Better outcome for suture button compared with single syndesmotic screw for syndesmosis injury: five-year results of a randomized controlled trial. Bone Joint J 2020;102-B(2):212-9.
- Lin X, Tu C, Lin W, et al: Comparison the treatment of anterior inferior tibiofibular ligament anatomical repair and syndesmosis screw fixation for syndesmotic injuries in ankle fracture. BMC Surg 2023;23(1):80.
- Kwon JY, Stenquist D, Ye M, et al: Anterior syndesmotic augmentation technique using nonabsorbable suture-tape for acute and chronic syndesmotic instability. Foot Ankle Int 2020;41(10):1307-15.
- Zhan Y, Yan X, Xia R, et al: Anterior-inferior tibiofibular ligament anatomical repair and augmentation versus trans-syndesmosis screw fixation for the syndesmotic instability in external-rotation type ankle fracture with posterior malleolus involvement: a prospective and comparative study. Injury 2016;47(7):1574-80.
- Teramoto A, Shoji H, Sakakibara Y, et al: Suture-button fixation and mini-open anterior inferior tibiofibular ligament augmentation using suture tape for tibiofibular syndesmosis.