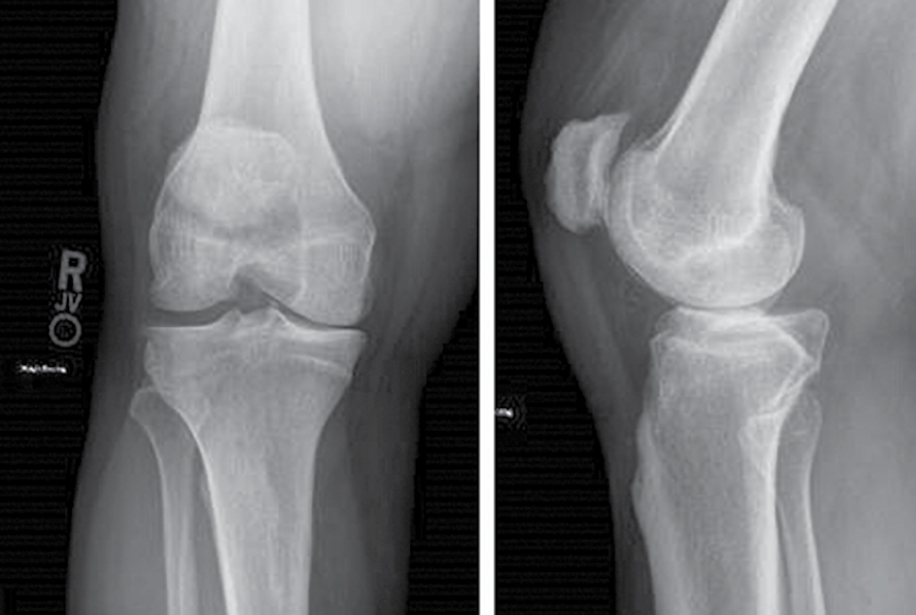
Fig. 1 Preoperative standing anteroposterior radiograph (left) and standing lateral radiograph (right) of a patient (male, aged 45 years) with medial-sided knee pain and no prior surgical intervention
Courtesy of Cassandra A. Lee, MD, FAAOS
Published 12/18/2024
|
Jared B. Watson, MD; Cassandra A. Lee, MD, FAAOS
Osteoarthritis (OA) is a leading cause of chronic pain and disability in adults. Of the global population of working-age adults between 30 to 60 years old, 3 to 5 percent live with some degree of OA. The management of a young and active individual with knee OA has been a long-standing challenge. This patient population tends to want to remain active after surgery in sporting or high-impact activities. As degenerative changes to the cartilage and meniscus progress, nonoperative treatment options often lose their effectiveness over time. A treatment gap exists for patients with knee OA who are unresponsive to conservative management but who are unwilling or are not quite ready for more invasive surgical procedures. An extra-articular implantable shock absorber (ISA) is a promising option to address the population of young and active individuals suffering from mild to moderate medial compartment knee OA (Figs. 1 and 2).
After failure of conservative management, surgical options for this patient population have historically been high tibial osteotomy (HTO) or arthroplasty (unicompartmental or total replacement). Each of these options presents significant limitations and risks. Risks associated with HTO include nonunion, tibial plateau fracture, persistent pain, and hardware complications. Furthermore, HTO transfers loads from the medial compartment laterally, potentially exacerbating or worsening lateral knee OA. Patients younger than 50 years who undergo total knee arthroplasty (TKA) are at significantly increased risk of requiring revision surgery due to prosthetic joint infection or aseptic loosening. A multicenter survey of 661 patients (aged <60 years) who underwent primary tka found that 50 percent of patients were unable to return to desired recreational activity. one-third of those patients reported residual pain. additionally, in a large cross-sectional study of patients undergoing primary tka (n=1,703 participants), nearly 20 percent of patients reported that they were not satisfied with outcomes of surgery. Of that patient population, patients younger than 70 years at the time of surgery were more likely to be dissatisfied.
Fig. 1 Preoperative standing anteroposterior radiograph (left) and standing lateral radiograph (right) of a patient (male, aged 45 years) with medial-sided knee pain and no prior surgical intervention
Courtesy of Cassandra A. Lee, MD, FAAOS
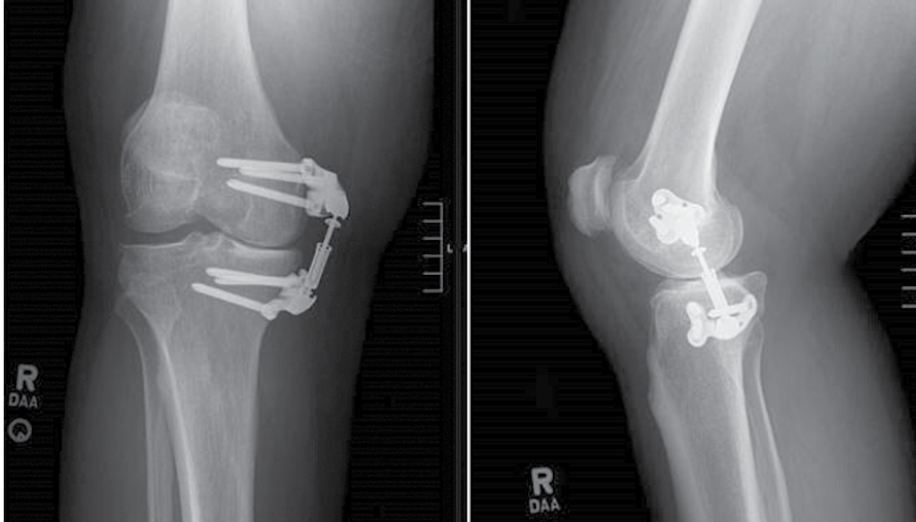
Fig. 2 Postoperative standing anteroposterior radiograph (left) and standing lateral radiograph (right) of a patient (male, aged 45 years) with medial-sided knee pain after implementation of an implantable shock absorber
Courtesy of Cassandra A. Lee, MD, FAAOS
An ISA utilizing a polymer for shock absorption is an alternative option in this population. It was developed in 2014 by Moximed, Inc., and called the Atlas Knee System. Over time, the initial Atlas Knee System has been redesigned and improved to its most recent iteration (the Calypso), which is placed subcutaneously into the medial extracapsular space, superficial to the medial collateral ligament to functionally unload the medial compartment of the knee. Its design consists of a cylindrical shock absorber fixed by titanium plates to the distal femur and proximal tibia. The ISA can reduce peak medial joint forces by more than 30 percent, equivalent to HTO, but does not transfer the load laterally and does not overload the lateral compartment.
The PHANTOM High Flex Trial was a single-arm prospective study that followed the 2-year postoperative outcomes of 26 subjects aged 25 to 65 years with at least 6 months of knee pain and mild to moderate medial knee compartment OA. Participants underwent implantation of the Atlas Knee System. No patients in the study underwent concomitant procedures during implantation of the Atlas system. At 1-year follow-up, 25 of 26 patients had retained implants. One implant was removed due to pain and stiffness of the knee. At 2-year follow-up, one subject had arthroscopic debridement and microfracture of a trochlear lesion, and another subject had arthroscopic meniscectomy and medial osteophyte removal. All 25 patients with retained hardware at 2 years reported meaningful improvement of knee pain, and 96 percent reported clinically improved function.
In the pivotal multicenter clinical trial of the Calypso implant (Diduch et al), 81 participants aged 25 to 65 years underwent ISA implantation. The ISA arm was compared to a historical control group of 81 patients treated with opening-wedge HTO. At 24 months, ISA was found to be superior to HTO in terms of pain and function, surgical complications, and conversion to arthroplasty or other joint-modifying surgery. Patients were able to return to full weight bearing sooner in the ISA group (13.4 days versus 58 days). Improvements in pain and function relative to baseline were also higher in the ISA group at both 3 and 24 months.
Adverse events were classified by the FDA’s Investigational Device Exemption clinical protocol. Overall, there were 15 device- and procedure-related serious adverse events (SAEs) in 13 participants in the ISA group (16 percent). In comparison, there were 42 SAEs in 37 participants in the HTO group (45.7 percent). SAEs were significantly higher in the HTO group, with pain being the primary contributor to the group differences (P <0.001). there were no mechanical device malfunctions in either group. there was one instance of screw backout in the isa group and one incidence of screw breakage in the hto group. the rate of secondary operations for implant removal was significantly lower in the isa group compared with the hto group (11 vs 61, respectively). one patient in the isa group was converted to arthroplasty. the other 10 subjects underwent implant removal without complication, with nine reporting sustained relief of medial compartment knee pain. it is worth noting that a significant number of secondary procedures in the hto group may have been performed electively after bone consolidation to prevent hardware complications in the future.
Conclusion
Symptomatic knee OA in the younger, high-demand patient population has been a challenging clinical scenario for orthopaedic surgeons. For the appropriate patients fitting into this “treatment gap,” ISA has been shown to be noninferior and even superior to previous treatment options for isolated medial compartment OA. HTO and ISA both were associated with low rates of adverse events; however, ISA subjects were able to mobilize 400 percent sooner; in addition, nearly 80 percent reported pain improvement at 24 months, and nearly 96 percent were considered responders for pain.
The long-term outcomes of ISA are yet to be investigated; however, ISA has shown promise as a less invasive alternative in short-term to midterm outcome studies. It is essential to appropriately counsel surgical candidates that implantation of a joint unloading device is not a cure for underlying disease. Pain is the most common adverse effect after this procedure. This finding is not surprising, given that candidates for this procedure are working-aged individuals with mild to moderate medial compartment arthritis. Prior patient preference studies have suggested that young, active individuals with knee OA will often tolerate pain if they can avoid bone-cutting treatments such as arthroplasty or HTO and maintain desired activities. Joint unloading devices such as ISA have a low risk profile and can serve as a bridge treatment for younger and active patients limited by pain due to medial knee compartment OA.
Jared B. Watson, MD, is a fourth-year orthopaedic surgery resident at the University of California, Davis (UC Davis)
Cassandra A. Lee, MD, FAAOS, is a professor and chief of orthopaedic sports medicine at UC Davis Health. Her clinical interests include joint preservation of the knee. Her research interests include modulation of post-traumatic OA.
References
- Dieleman JL, Baral R, Birger M, et al: US spending on personal health care and public health, 1996–2013. JAMA 2016;316:2627.
- Cieza A, Causey K, Kamenov K, et al: Global estimates of the need for rehabilitation based on the Global Burden of Disease Study 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2021;396(10267):2006-17.
- Liu X, Chen Z, Gao Y, et al: High tibial osteotomy: review of techniques and biomechanics. J Healthc Eng 2019;2019:8363128.
- Meehan JP, Danielsen B, Kim SH, et al: Younger age is associated with a higher risk of early periprosthetic joint infection and aseptic mechanical failure after total knee arthroplasty. J Bone Joint Surg Am 2014;96(7):529-35.
- Parvizi J, Nunley RM, Berend KR, et al: High level of residual symptoms in young patients after total knee arthroplasty. Clin Orthop Relat Res 2014;472:133-7.
- Bourne RB, Chesworth BM, Davis AM, et al: Patient satisfaction after total knee arthroplasty: who is satisfied and who is not? Clin Orthop Relat Res 2010;468:57-63.
- London NJ, Miller LE, Block JE: Clinical and economic consequences of the treatment gap in knee osteoarthritis management. Med Hypotheses 2011;76(6):887-92.
- Krummenauer F, Wolf C, Günther KP, et al: Clinical benefit and cost effectiveness of total knee arthroplasty in the older patient. Eur J Med Res 2009;14(2):76-84.
- Morgan OJ, Hillstrom HJ, Ranawat A, et al: Effects of a medial knee unloading implant on tibiofemoral joint mechanics during walking. J Orthop Res 2019;37(10):2149-56.
- Diduch DR, Crawford DC, Ranawat AS, et al: Implantable shock absorber provides superior pain relief and functional improvement compared with high tibial osteotomy in patients with mild-to-moderate medial knee osteoarthritis: a 2-year report. Cartilage 2023;14(2):152-63.
- Slynarski K, Walawski J, Smigielski R, et al: Two-year results of the PHANTOM High Flex Trial: a single-arm study on the Atlas Unicompartmental Knee System load absorber in patients with medial compartment osteoarthritis of the knee. Clin Med Insights ArthritisMusculoskelet Disord 2019;12:1179544119877170.
- Pareek A, Parkes CW, Gomoll AH, et al: Improved 2-year freedom from arthroplasty in patients with high-risk SIFK scores and medial knee osteoarthritis treated with an implantable shock absorber versus non-operative care. Cartilage 2023;14(2):164-71.
- Slynarski K, Walawski J, Smigielski R, et al. Feasibility of the Atlas Unicompartmental Knee System load absorber in improving pain relief and function in patients needing unloading of the medial compartment of the knee: 1-year follow-up of a prospective, multicenter, single-arm pilot study (PHANTOM High Flex Trial). Clin Med Insights Arthritis Musculoskelet Disord 2017;10:1179544117733446.
- Bode G, Kloos F, Feucht MJ, et al: Comparison of the efficiency of an extra-articular absorber system and high tibial osteotomy for unloading the medial knee compartment: an in vitro study. Knee Surg Sports Traumatol Arthrosc 2017;25(12):3695-703.
- Losina E, Katz JN: Total knee arthroplasty on the rise in younger patients: are we sure that past performance will guarantee future success? Arthritis Rheum 2012;64(2):339-41. doi: 10.1002/art.33371.
- Moorman CT, III, Kirwan T, Share J, et al: Patient preferences regarding surgical interventions for knee osteoarthritis. Clin Med Insights Arthritis Musculoskelet Disord 2017;10:1179544117732039.