Robotic Assisted Bi-Cruciate Retaining Total Knee Arthroplasty: Physiological Alignment Due to Avoid “Kinematic Conflict”
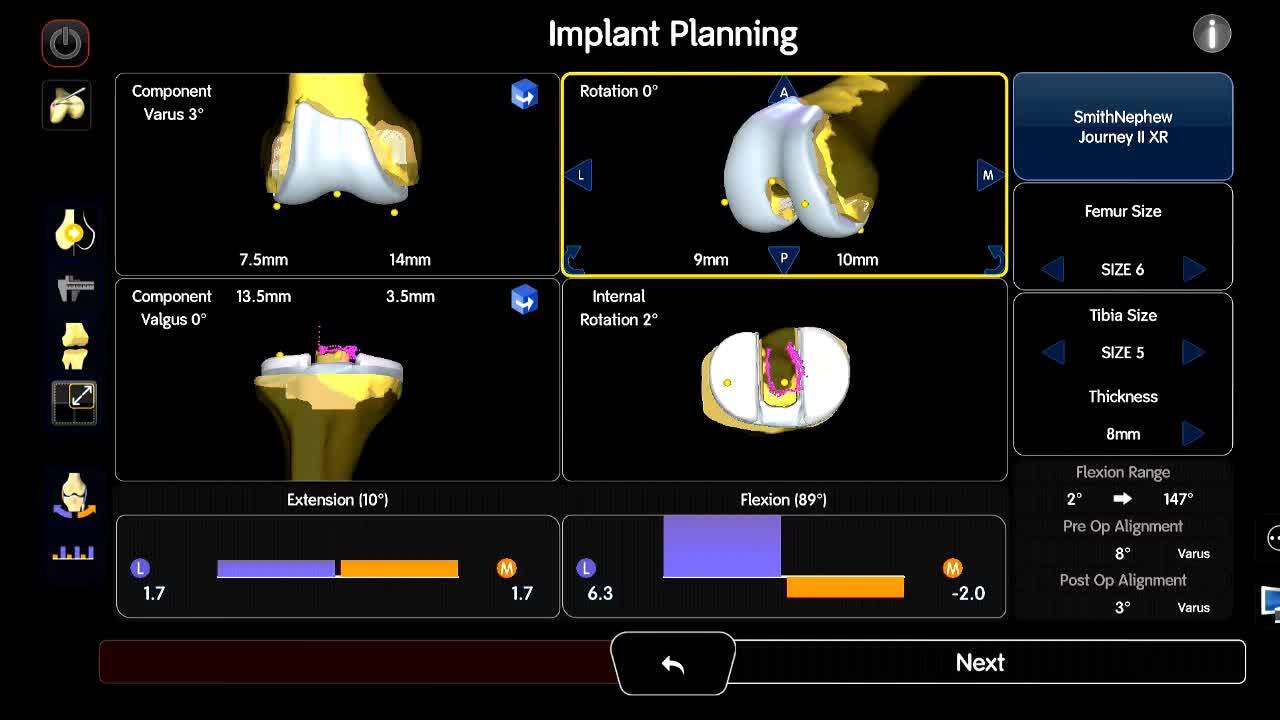
Background: The majority of current TKA designs sacrifice the anterior cruciate ligament (ACL) without substituting for its function. The loss of the ACL has significant effects upon the kinematics of the knee, recently, bi-cruciate retaining (BCR) TKA is again attracting attention. Fluoroscopic imaging has demonstrated contact points in full extension, as well as posterior rollback at 90° flexion that more closely replicates the normal knee. However, the first-generation BCR TKAs, namely the polycentric knee and geometric knee, are complicated techniques that cause what is known as a “kinematic conflict,” where ligamentous tension increases at certain flexion angles due to the preservation of all ligaments, resulting in early post-operative revision. Recently, novel robotic-assisted technology (handheld image-free RA surgical systems. NAVIO® and CORI®, Smith & Nephew, Plymouth, MN, USA) make it possible to intra-operatively determine component alignment and the amount of damaged osteochondral cartilage to be removed while considering soft tissue balancing over the full range of motion. This RA technique is expected to improve patient-reported outcome measurements (PROMs) with the second-generation Journey II XR (asymmetry, XR, Smith & Nephew, Inc., Memphis, TN, USA).Purpose: This video demonstrates a RA technique for physiological alignment using second generation BCR prosthesis, due to avoid kinematic conflicts.Methods: The case presentation of a 76-year-old female with two compartmental Knee (medial femoral/tibial and patella-femoral OA) is reviewed. The mechanically alignment was set as the target alignment using a pre-operative 3DCT- based system. The most beneficial feature of RA system was that planning for prosthesis size, component alignment, and osteochondral resection volume was modified based on the soft tissue envelope of each patient over the full ROM using an intra-operative joint-balancing procedure. We have previously reported that achieving the slightly laxity medial joint gap (MJG) from 0° to 140° of flexion, the tightness of the lateral joint gap (LJG) at 90° of flexion and a physiological laxity (MJG < LJG) from 0° to 140° of flexion results in improved postoperative PROMs when utilizing Journey ? XR with a balancer. Therefore, in the RA surgical technique, the prosthetic alignment and osteotomy volume were determined by considering the soft tissue envelope with reference to these.Results: The physiological alignment with intra-operative MJG (2.1mm, 2.2mm) and LJG (2.2mm, 6.2mm) in extension and at 90° of flexion could be achieved. Intra-operative flexion angle was 152° and tibial internal rotation angle in intra-operative kinematics was 17°, equivalent to a healthy knee.Conclusion: Physiological alignment with RA BCR TKA does not cause kinematic-conflict.