Anterior Cruciate Ligament Reconstruction With Synthetic Augmentation and Lateral Extra-articular Tenodesis for High-Grade Anterior Cruciate Ligament Instability
The patient shown in this video is a 31-year-old man who has experienced 7 weeks of left knee pain after jumping from a height of 2 to 4 feet. The patient reported feeling as if his knee dislocated on impact. Since the injury, the patient has experienced anterior knee pain, intermittent swelling and instability, catching, and locking. Previous attempts at a home exercise program, cryotherapy, and over-the-counter medications have been unsuccessful in managing the patient’s pain and instability.
Physical examination of the left knee revealed a mild effusion, with a grade 2 anterior drawer test, tenderness to palpation at the medial joint line, a grade 2B Lachman test, guarding with the pivot shift test, normal patellar tracking, and normal quadriceps and hamstring strength. MRIs of the left knee showed evidence of an anterior cruciate ligament injury. Posteromedial edema with a posteromedial meniscus tear, likely complex with horizontal-in-vertical components, and medial meniscus extrusion were observed.
The patient was placed on the surgical table in the supine position. An examination under anesthesia confirmed instability with rotational laxity and a considerable pivot shift. A standard, medial midline incision was made over the left anterior knee, and the paratenon was incised, exposing the patellar tendon. The central third of the patellar tendon was harvested (approximately 10 mm in width). A tapered graft was created, with 20 mm taken on the patellar side and 25 to 30 mm taken on the tibial aspect. Bone blocks were cut from the patella and tibia and fashioned to a width of approximately 9 mm to ensure appropriate placement in the tunnel. The graft was removed and placed under tension on the back table. After graft harvest, diagnostic arthroscopy proceeded.
Standard medial and lateral portals were created. Synovitis was observed in the suprapatellar pouch, which was débrided along with the anterior cruciate ligament remnant. Initial evaluation of the medial meniscus revealed a tear in the red-white zone. The lateral meniscus showed a complex tear that was determined to be irreparable; therefore, it was débrided to a stable base. With the knee in 115° of hyperflexion, the anatomic footprint on the lateral femoral condyle was exposed for the femoral tunnel. The guide pin was drilled into place in the femoral tunnel and was found to be in acceptable position. The femoral tunnel was subsequently over-reamed with the use of a 9-mm reamer, and a traction suture was passed through the tunnel. Drilling the femoral tunnel through the anteromedial aspect of the intercondylar ridge allows for more anatomic placement of the graft and better rotational stability.
Attention was then shifted to tibial tunnel placement. The guide was set to 55° at the anterior cruciate ligament tibial footprint in line with the medial tibial spine and at the posterior margin of the anterior horn of the lateral meniscus. Acceptable positioning of the tibial tunnel was confirmed, and the tunnel was subsequently over-reamed with the use of a 9-mm reamer, after which the traction suture was withdrawn through the tibial aperture. The femoral sided graft sutures and the internal brace were placed through the passing suture. The graft suture (black) and the internal brace sutures (white and blue) were visualized in the femoral tunnel. The button to the internal brace was passed through the tunnel and secured to the lateral aspect of the femur. Tension was applied distally on the sutures to ensure adequate fixation. The graft was then deployed and secured in place. After the graft was confirmed in the appropriate position, a notch was created in the femoral tunnel in preparation for screw fixation. The femoral screw applicator was placed in the femoral tunnel in a protective sheath to prevent damage to the anterior cruciate ligament graft and the posterior cruciate ligament. Tension was placed on the distal end of the graft suture to ensure appropriate fixation.
Attention was then shifted to medial meniscus repair with the use of three alternating all-inside meniscal fixators. A probe was placed under the internal brace to prevent over-tensioning. This serves as a checkrein or seatbelt to the anterior cruciate ligament rather than a primary source of restraint. After meniscal repair, the sutures for the internal brace and graft were separated. The knee was placed in full extension, and a screw was placed to fix the distal end of the graft to the tibia. A hole was drilled just distal to the tibial tunnel. The cortex of the tibia was tapped, and the anchor was deployed for distal fixation of the internal brace and the anterior cruciate ligament graft.
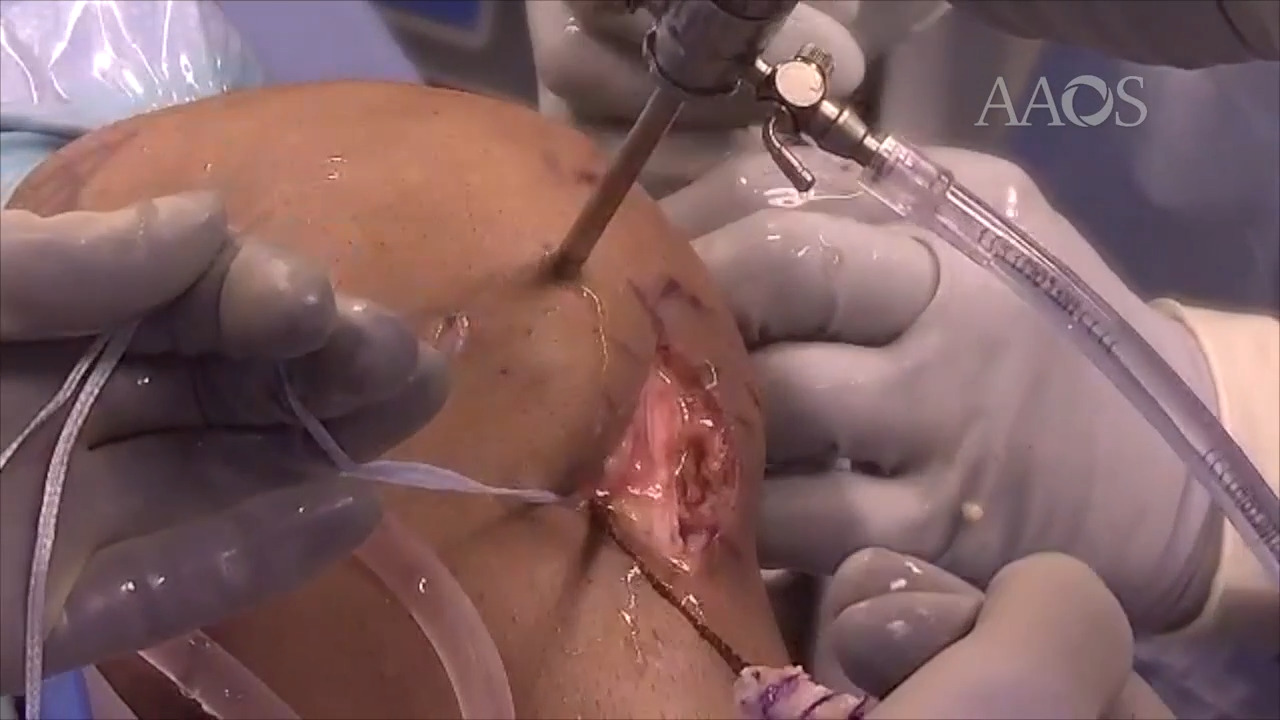
Given the patient’s asymmetric hyperextension, high-grade pivot shift test, and primary anterior cruciate ligament failure, the authors of the video elected to perform extra-articular tenodesis with the use of the iliotibial band. An incision was made over the lateral aspect of the iliotibial band between the Gerdy tubercle and the lateral femoral epicondyle. A central 10-mm band of the anterocentral iliotibial band was released and harvested at approximately 8 cm in length and left intact distally. Using suture, a whipstitch was created around the released graft. The graft was released and freed distally. The lateral collateral ligament was identified and exposed via blunt dissection with the use of a hemostat. With the knee flexed to 30° in neutral rotation, the graft was fixed to the femur posteriorly and proximally with the use of a knotless self-punching anchor. Keeping the anterior cruciate ligament graft suture in place helps avoid the femoral tunnel. The graft was then sewn back onto itself with the use of a free needle.
Outcomes observed in studies using suture tape reinforcement as an internal brace in anterior cruciate ligament reconstruction reported a 7.4% re-tear rate in the group with internal bracing and a 13.8% re-tear in the group without internal bracing. In addition, studies on lateral extra-articular tenodesis with anterior cruciate ligament reconstruction have shown decreased anterior tibial translation and reduced tibial internal rotation, which typically results in anterolateral instability and may lead to anterior cruciate ligament graft failure.
Postoperative management includes ambulation in a hinged knee brace and with the use of crutches, physical therapy, and the use of an assistive device for walking for 6 to 8 weeks postoperatively. Anticipated return to physical activity is 7 to 8 months postoperatively.