Rotationplasty: Technique for Osteosarcoma of the Distal Femur in a Young Child
This video demonstrates the technique for rotationplasty in a young child with osteosarcoma using an intramedullary nail. Treatment considerations, indications, risks of surgical management, and technique are discussed.
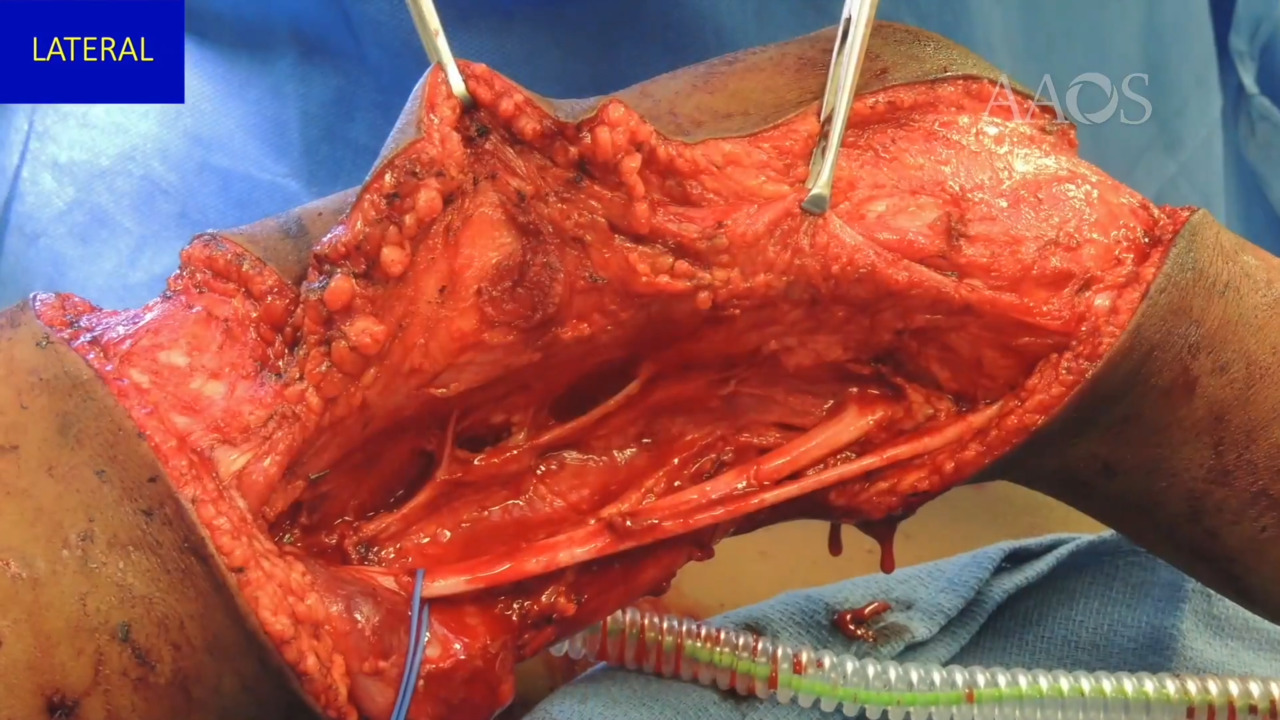
A rhomboid skin incision is marked, with the anterior long axis approximately 5 cm longer than the intended bone cuts. Limb-length measurements are then made to confirm preoperative calculations and mark the anterior aspect of the skin longitudinally to aid in limb rotation later in the procedure. The approach is started sharply and carried down to the subcutaneous tissues. Electrocautery is performed more deeply to attain hemostasis. After soft-tissue flaps are elevated circumferentially, lateral dissection is carried out with the use of Metzenbaum scissors to identify the common peroneal nerve posterior and medial to the distal biceps femoris. This is then protected with the use of a vessel loop. The peroneal nerve is traced proximally to locate the tibial branch of the sciatic nerve, which also is protected.
Next, attention is shifted medially, identifying the vastus medialis and the adductor magnus, which is transected to allow for exposure of the vessels. Doppler is used to localize the vessels for additional dissection. The saphenous vein is ligated with the use of suture. After the vessels are identified and protected with the use of a vessel loop, the numerous perforating branches to the tumor are ligated with the use of clips or silk suture. This is performed until the vessels are free for the length of the anticipated bony resection. Next, Kirschner wires are placed in the tibia and femur, widely outside the zone of resection, to aid with rotation later in the procedure. The extensor mechanism is transected, after which the cruciate ligaments, collateral ligaments, and posterior capsule are released. Any remaining hamstring muscles are released. The gastrocnemius muscles are transected at the level of the joint, and the popliteus is released from the tibia, leaving a wide cuff of tissue with the tumor. Proximally, the remaining quadriceps muscle is released to expose the femur in preparation for osteotomy. After the femur is transected with the use of a saw, the remaining soft-tissue attachments are released, and the distal femur and the adjacent soft tissues are lifted out of the surgical field. At this point, the specimen is grossly inspected to confirm no visible tumor. In addition, a frozen section of the bone marrow at the femur can be performed proximally to confirm no residual tumor remains. Approximately 3 cm of proximal tibia is removed, and the fibula is resected just below the level of the physis. A combination of curets and a high-speed burr are used to clear a space wide enough to allow for intussusception of the remaining femur and proximal tibia. The tibia is then externally rotated 180° and intussuscepted.
Next, attention is shifted to the femur for intramedullary nail placement. Before incising the proximal femur, the nail and guidewire can be laid over the femur and tibia to ensure a nail of the appropriate size and length is available. Next, the starting point for a lateral entry nail is attained and confirmed via fluoroscopy. The intramedullary nail is placed after standard reaming technique. Before placement of interlocking screws, the vessels are assessed and confirmed to have distal flow via Doppler. Distal interlocking screws are then placed via perfect-circle technique.
Attention is then shifted to closure. Overly tight closure of the deep soft-tissue layers is avoided because of the risk of undue compression of the vessels. A small area of tissue is cleared to accommodate coiling of the femoral vessels. Papaverine is used to help with vasospasm, and pulses are confirmed after closure of the skin with the use of nylon suture. Postoperatively, the patient has done well, restarted chemotherapy, and begun fitting for a prosthesis for ambulation.