Elbow Ulnar Collateral Ligament Repair Using Suture Augmentation, Anchors, and Bone Tunnels
Ulnar collateral ligament (UCL) repair with suture augmentation has been increasingly performed to manage UCL pathology in overhead athletes. In appropriately indicated patients, UCL repair with suture augmentation but without reconstruction is associated with promising results. Advantages of repair with suture augmentation include earlier return to sports activity, low complication rate, and decreased surgical time because graft harvest is not necessary. Previously reported techniques involve suture anchors with high-tensile and collagen-coated nonabsorbable sutures. This article provides an alternative augmentation method involving a combination of anchors and bone tunnels to attain isometric repair.
Technique
Patient Positioning
The patient is placed in a supine position and administered general anesthesia. A standard hand table attachment is used, and a sterile tourniquet is applied high on the arm. A 6- to 8-cm incision is marked, centered over the medial epicondyle. The ulnar nerve is palpated and marked posterior to the medial epicondyle. A careful physical examination is performed to ensure the nerve does not sublux or dislocate with elbow range of motion. An Esmarch bandage is applied, and the tourniquet is inflated.
Surgical Exposure
The incision is made through the skin and dermis. Superficial dissection is carried down through the subcutaneous tissues with the use of bipolar cautery. The medial antebrachial cutaneous nerve and/or branches are identified and protected. The medial intermuscular septum is identified and released from the medial epicondyle. The fascia over the common flexors is identified and incised between the two heads of the flexor carpi ulnaris in line with the muscle fibers. The flexor carpi ulnaris is split and bluntly dissected to expose the entire length of the underlying UCL from the sublime tubercle to the medial epicondyle. The substance of the UCL is then evaluated for its quality and integrity. If there is considerable attrition of the UCL, then the patient may be better served with reconstruction. If the quality of the tissue is deemed appropriate, the repair is continued with suture augmentation. The substance of the UCL is then incised from the sublime tubercle to the medial epicondyle, exposing the ulnohumeral joint.
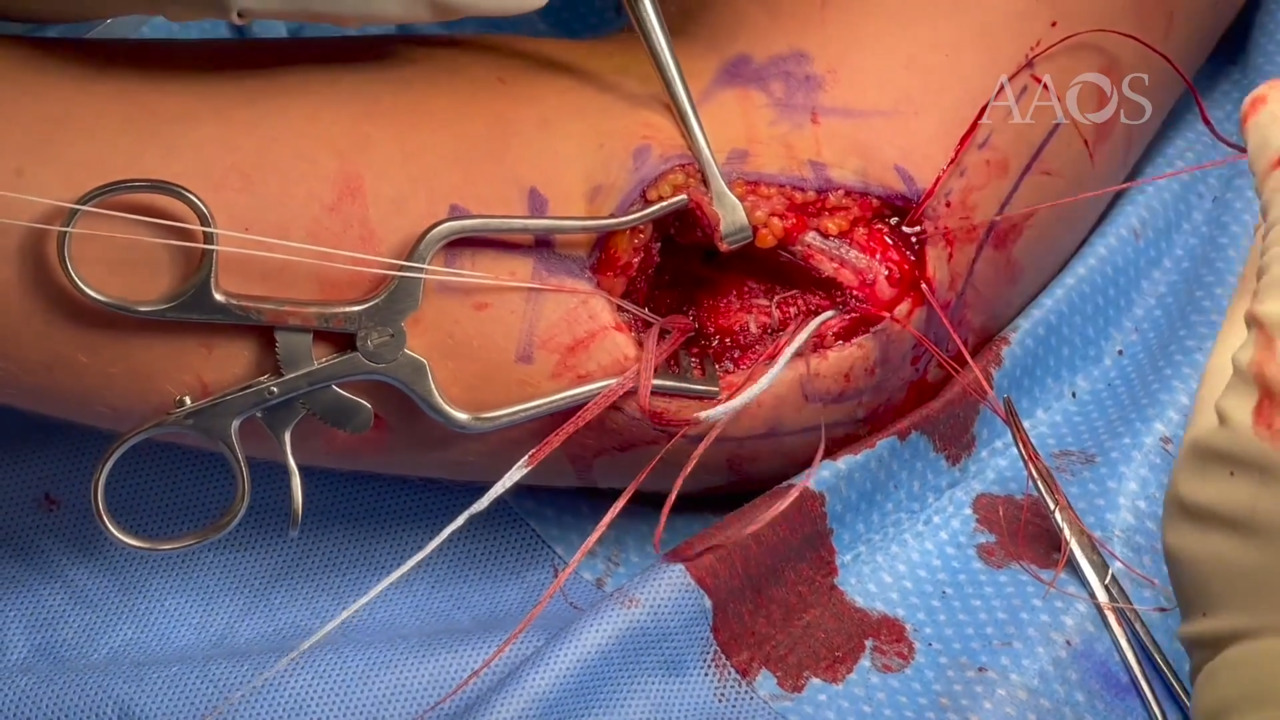
UCL Repair and Suture Augmentation
Attention is then turned to the UCL insertion at the sublime tubercle, at which overlying soft tissue and periosteum is débrided. Care is taken to identify and preserve the ulnar nerve, which is directly posterior to the sublime tubercle. A 3.5-mm nonabsorbable suture anchor loaded with 2-mm collagen-coated FiberTape (Arthrex) and No. 0 FiberWire (Arthrex) is placed at the UCL attachment at the sublime tubercle. Next, attention is shifted to the medial epicondyle. A 3.5-mm drill hole closed tunnel is then made in the elbow of the medial epicondyle, directed proximally. Care is taken to ensure this 3.5-mm tunnel is only unicortical. Next, two converging 2.5-mm drill holes are created from proximal to distal to converge with the 3.5-mm closed tunnel in a fashion similar to that for the humeral docking technique for UCL reconstruction. The two 2.5-mm tunnels that are created to converge with the central 3.5-mm tunnel are created so that one tunnel is medial and the other tunnel is anterior. The tunnels are created so an adequate bone bridge of at least 15 mm is present between the tunnels. If the surgeon plans to transpose the ulnar nerve anteriorly, then the two tunnels are placed more posteriorly so the suture knots are further from the anteriorly transposed nerve. A Hewston suture passer is used to pass a 2-0 Vicryl suture throughout each bone tunnel, with the loop of the suture exiting distally through the larger 3.5-mm drill hole to serve as shuttle suture later. A SutureTape (Arthrex) suture (0.9 mm) is then passed through the already incised native UCL tissue from distal to proximal in a locking Krakow fashion. One limb of the SutureTape (that was passed through the native UCL) and one limb of the FiberTape (from the 3.5-mm nonabsorbable suture anchor in the sublime tubercle) are passed through one of the tunnels with one set of the shuttle sutures (Vicryl). The other remaining SutureTape limb and FiberTape limb are passed through the other tunnel with the other shuttle suture. The elbow is held in 50° of flexion via a varus force with the forearm in supination. The limbs of the FiberTape are first tied together with alternating half-hitch knots over the bone bridge over the medial epicondyle. The elbow is ranged to ensure adequate isometry and that full flexion is achieved. The SutureTape limbs are then also tied together. The native UCL is oversewn with the use of 3-0 Vicryl for additional tensioning. The No. 0 FiberWire from the 3.5-mm nonabsorbable suture anchor in the sublime tubercle is then used to repair the distal end of the native UCL.
Wound Closure
The flexor carpi ulnaris fascia is repaired with the use of 3-0 Vicryl in-running or interrupted sutures. The wound is then closed in layers based on surgeon preference, and the elbow is splinted in approximately 80° of elbow flexion.
Rehabilitation
The arm is immobilized for 7 to 10 days, after which a hinged elbow brace is applied. Active range of motion is initiated at 2 weeks postopertively, with 15° of locked extension, and full range of motion and strengthening are initiated at 4 weeks postoperatively. An interval throwing program is initiated at 3 to 4 months postopertively with a goal of return to play at 6 to 7 months postopertively.
Conclusion
This video demonstrates an additional method for UCL repair with internal brace management of acute and subacute UCL injury. In the experience of the authors of this video, this technique is associated with a high rate of return to play with few complications; however, additional biomechanical and clinical studies are necessary to validate this method.