Anterior Cruciate Ligament Repair: Rationale and When to Consider Over Reconstruction
Background
Anterior cruciate ligament (ACL) restoration is divided into repair versus reconstruction. This video demonstrates ACL repair with the fixation of an adjustable cortical button on the femur.IndicationsACL rupture is a condition in which restoration is essential to regaining adequate knee function. ACL repair may be indicated in patients with an acute tear (<4 weeks), patients with a Sherman type I or type II tear, patients aged 35 years or older, and patients with a mild to moderate activity level.
Technique Description
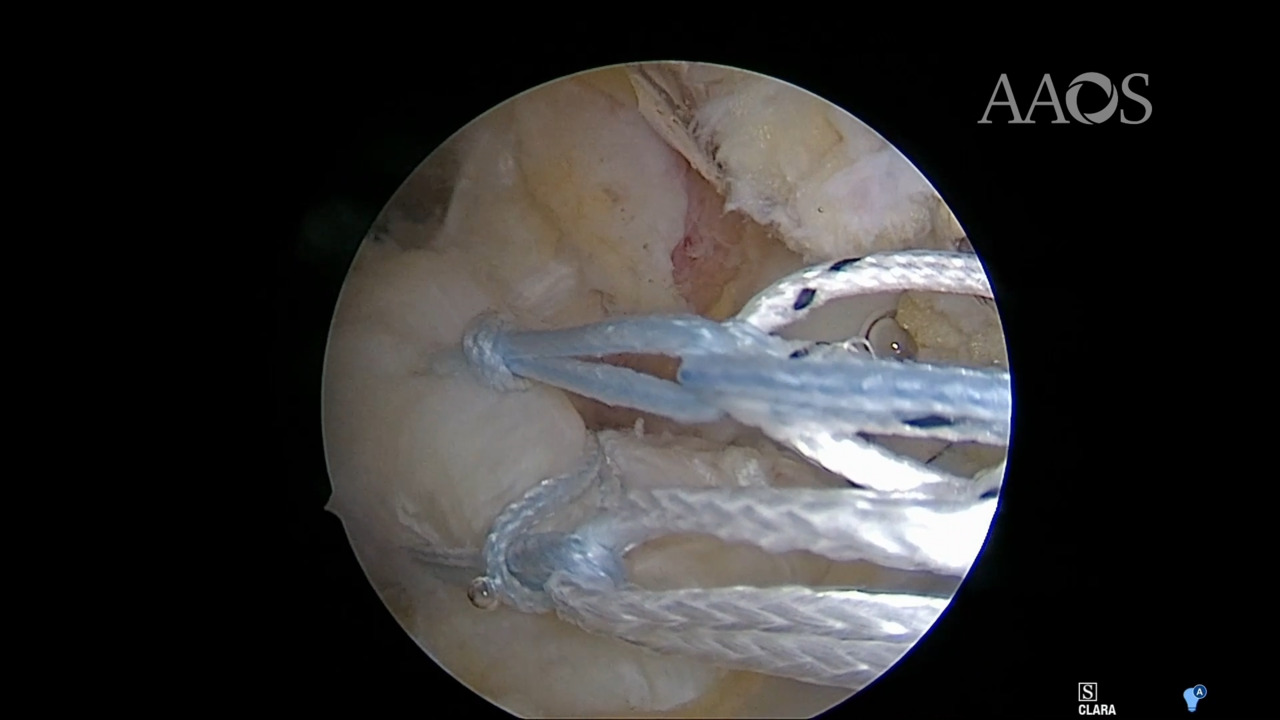
ACL tightrope repair initially requires identification of the ACL tear. The femoral wall is then prepared, and a drill tunnel is created in the femoral and tibial walls. FiberRing sutures (Arthrex) are passed through the intact portion of the ACL as many times as desired. An ACL Tightrope (Arthrex) is then fed through the FiberRing sutures. The ACL Tightrope and a cortical button are passed through the femoral tunnel. FiberTape sutures (Arthrex) are passed through a tibial tunnel to act as an internal brace. Range of motion and tension are assessed and adjusted as necessary.
Results
Patients who meet the indications for ACL repair and undergo repair via a Tightrope implant may have outcomes comparable to those of patients who undergo ACL reconstruction. Patient-completed functional knee scores, such as the International Knee Documentation Committee score, Knee Injury and Osteoarthritis Outcome Score, and Lysholm Knee Scale score, are similar between the two restoration techniques; however, younger patients who undergo ACL repair appear to have a higher failure rate with Tightrope implants compared with reconstruction.
Conclusion
ACL repair may be an adjuvant treatment option in patients with an acute femoral sided tear. Caution should be exercised in performing this procedure in younger, higher level athletes. The use of an adjustable cortical button minimizes bone loss on the femoral wall while providing adequate fixation.