Chronic Proximal Tibiofibular Joint Instability: Cortical Button Fixation
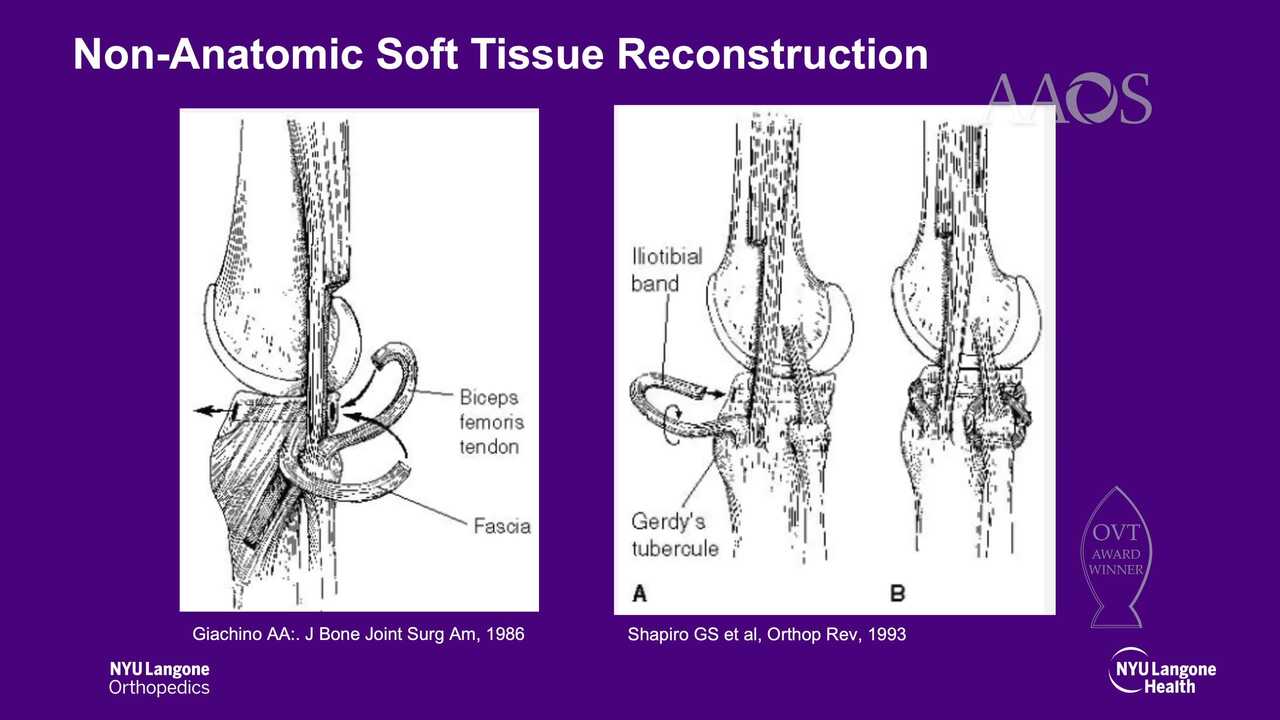
Background Instability of the proximal tibiofibular joint (PTFJ) is a rarely reported condition that can be easily missed or confused with more common lateral knee pathology; however, unmanaged instability of the PTFJ can lead to considerable disability. Although nonsurgical treatment may be sufficient, a large percentage of patients with chronic instability will continue to experience symptoms and ultimately require surgical treatment. Currently, the optimal surgical treatment option for patients with chronic PTFJ instability is unknown. Fixation methods include metal implants, autograft, allograft, and dynamic suture button devices. Described techniques include anatomic and nonanatomic reconstruction of the proximal tibiofibular ligaments, direct ligamentous repair, internal fixation, and PTFJ arthrodesis with fibular head resection. Fixation with the use of a suture button may restore normal PTFJ motion and stability without requiring graft harvest or secondary hardware removal.
Purpose
This video provides an overview of PTFJ reconstruction with adjustable-loop cortical button fixation for the management of chronic PTFJ instability.
Methods
The anatomy, physical examination, diagnosis, and treatment options for PTFJ instability are reviewed. The case presentation of a 40-year-old man with 1.5 years of recurrent PTFJ dislocations of the left knee is reviewed. The injury occurred during jiu-jitsu. Since the injury, the patient has experienced constant snapping of the fibula with occasional locking of the knee. The patient underwent initial osteochondral allograft and lateral meniscus repair of the left knee 8 months postinjury; however, he continued to experience instability symptoms and presented for a second opinion. After a thorough discussion of the risks, advantages, and prognosis, the patient elected to proceed with PTFJ reconstruction with cortical button fixation.
Results
PTFJ stability was restored intraoperatively. Good resolution of symptoms and full range of motion were observed at 6 weeks postoperatively. At 3 months postoperatively, the patient reported no recurrent dislocations.
Conclusion
PTFJ reconstruction with cortical button fixation is a viable surgical treatment option for PTFJ instability. This treatment option is associated with functional results similar to those of PTFJ reconstruction with the use of autograft or allograft, with less surgical morbidity.