Total Hip Arthroplasty via the Posterolateral Approach in Extreme Varus Deformity of the Proximal Femur
Introduction
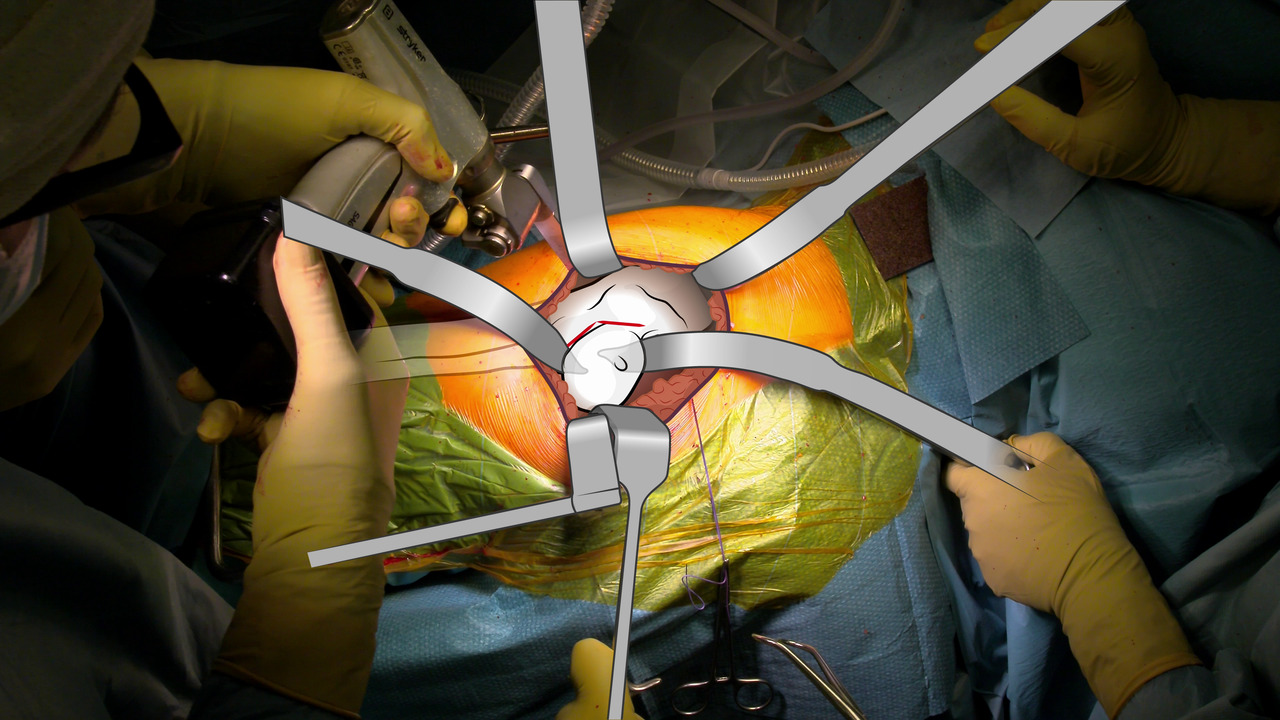
Despite the increasing popularity of the direct anterior approach for total hip arthroplasty (THA) in patients with severe hip osteoarthritis, the posterolateral approach still has relevance in the management of specific pathologies. The posterolateral approach offers numerous advantages, enabling surgeons to achieve optimal outcomes while ensuring the safety and well-being of their patients. This video explores the merits and advantages of the posterolateral approach in successfully removing endomedullary implants and fixation devices and in addressing severe deformities, such as a varus neck or posterior slippage of the femoral head, along with retraction of the posterior capsule. The goal of this video is to demonstrate the posterolateral approach for THA in a patient with secondary osteoarthritis associated with a varus neck and a severe flexion deficit.
Material and Methods
A retrospective review of 52 patients (58 hips) with secondary osteoarthritis and various degrees of varus neck deformity who underwent posterolateral THA between January 1, 2019, and May 28, 2022, was performed. Concurrent removal of fixation devices was performed in 38 of the 58 hips. Patient data, American Society of Anesthesiologists scores, surgical time, Harris Hip Scores, cup inclination, and stem alignment were assessed on postoperative radiographs. Intraoperative and postoperative complications up to 12-month follow-up were recorded. Group comparisons were conducted via Student t-test and chi-square analysis, with significance set at a P value of < 0.05.
Results
The mean patient age at the time of surgery was 54 years (range, 32 to 83 years). A significant improvement in Harris Hip Scores was observed, increasing from a mean of 41.5 points (range, 24 to 59 points) to a mean of 88.7 points (range, 78 to 96 points; P = 0.029), with resolution of flexion deficits in all the patients because of release of the posterior capsule. Radiographic evaluation revealed appropriate cup placement in the safe zone (40° ± 10°) in all the patients, with a mean of 37.9° of abduction. With regard to stem alignment, a mean of 0.3° varus positioning was observed. The complication rate was 6.8% (4 of 58 hips), consisting of two intraoperative femur fractures (both managed via cerclage wires), one wound infection managed via wound exploration, and one hip with aseptic loosening of the stem managed via revision surgery.
Discussion
The posterolateral approach for THA is a highly advantageous surgical technique and is particularly advantageous in patients with a history of hip surgery, femoral fixation devices, or a severe varus femoral neck deformity. The possibility of using a long stem is a key advantage of the posterolateral approach. In addition, the approach affords extensive access to the entire femoral shaft, enabling the surgeon to accurately address complex anatomic challenges. Another considerable benefit involves the effective and safe management of posterior capsule or gluteal retraction, thereby addressing flexion deficits. This is especially valuable in patients who have undergone previous hip surgery because it allows for precise correction of any existing problems while minimizing the risk of complications.
Conclusion
Despite the increasing popularity of the anterior approach for THA, the importance of the posterolateral approach must be recognized. The posterolateral approach should remain an essential skill in the surgical repertoire of hip replacement surgeons for the treatment of select patients.