Surgical Hip Dislocation and Femoral Head Osteochondral Allograft Transplantation
Background
Osteochondritis dissecans (OCD) of the femoral head is a rare condition, with limited studies available in the literature. Typically, OCD presents in the pre-teenage years. The knee is the most common location of OCD, whereas OCD of the femoral head is relatively uncommon, accounting for approximately 2% of all cases. Treatment options are based on skeletal maturity and lesion stability, ranging from nonsurgical management to hip arthroscopy and surgical hip dislocation, which affords the most extensive exposure of the acetabulum and the femoral head. The key to performing safe surgical hip dislocation is understanding that the blood supply to the femoral head comes from the terminal retrograde retinacular branches of the deep branch of the medial femoral circumflex artery and is protected by an intact obturator externus during the dislocation maneuver. This is a reliable technique with a low risk of osteonecrosis, nerve injury, infection, and fracture. Osteochondral allograft is a viable surgical treatment option, resulting in good short-term outcomes in the hip joint.
Purpose
This video demonstrates the safe surgical hip dislocation technique and osteochondral allograft transplantation for OCD of the femoral head in a skeletally immature patient.
Methods
The anatomy of, pathogenesis of, diagnosis of, and treatment options for OCD of the femoral head are reviewed. The case presentation of a 13-year-old male competitive fencer with pain in the right buttock and groin is reviewed. The patient's discomfort was initially diagnosed as a muscle strain. The patient underwent a trial of activity modifications and rest. After a thorough discussion of the risks, advantages, and prognosis of surgical treatment, the patient and his family elected to undergo surgical hip dislocation and osteochondral allograft transplantation to improve his pain and functional status.
Results
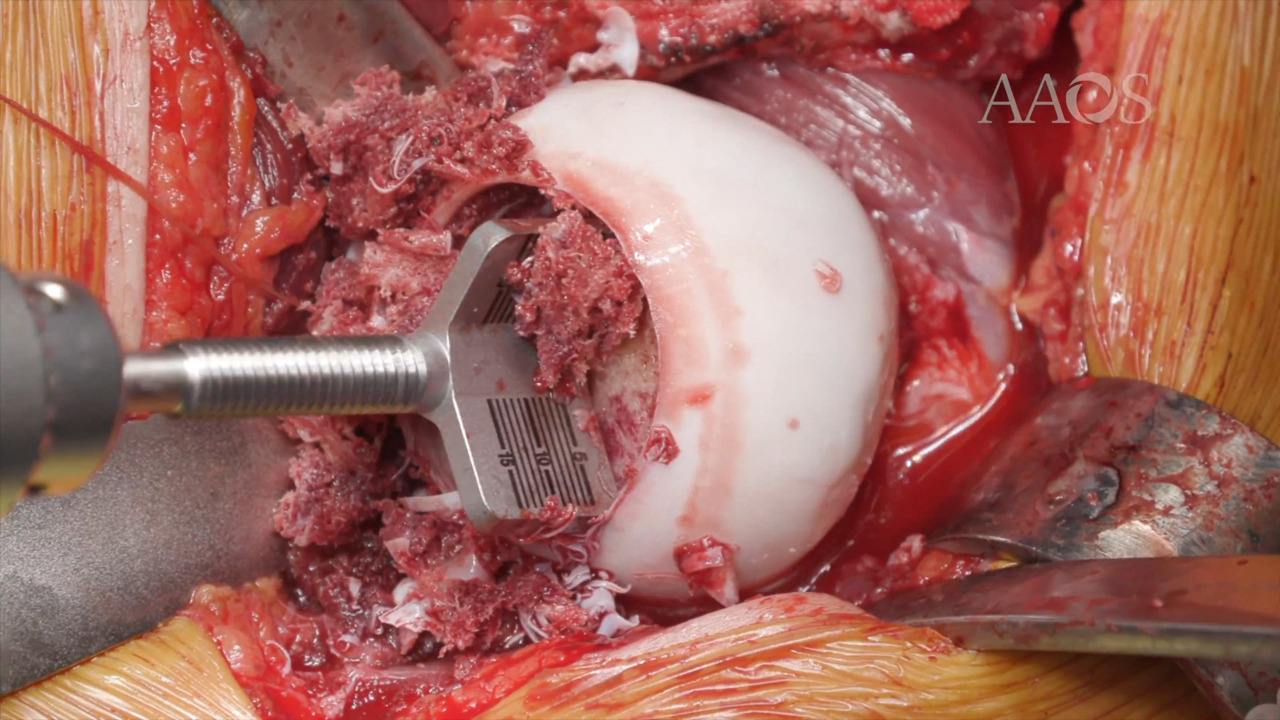
The hip joint was dislocated anteriorly after a greater trochanteric step-cut osteotomy was performed, with protection of the abductors, vastus lateralis, and short external rotators. The pathologic lesion was located, and successful osteochondral allograft transplantation was performed. The osteotomy and allograft showed signs of healing at 6 months postoperatively, and the patient returned to full activities without discomfort.
Conclusion
Surgical hip dislocation and osteochondral allograft transplantation is a viable surgical treatment option for skeletally immature patients with OCD of the femoral head. This treatment option can be performed in a single stage in patients with epiphyseal pathology incorporating more than 50% of the articular margin. Because of the experience of the two surgeons involved, this technique resulted in a good functional outcome with minimal surgical morbidity. Adherence to postoperative rehabilitation is crucial for optimal outcomes.