Supercharge End-to-Side Anterior Interosseous Nerve to Ulnar Motor Nerve Transfer
Supercharge end-to-side anterior interosseous nerve (AIN) to ulnar motor nerve transfers have increased in popularity over the past decade as a method to enhance intrinsic recovery. The supercharge nerve transfer facilitates nerve regeneration from the donor to the recipient via a perineural window, enhancing regeneration from the proximal regenerating nerve. The exact surgical method is difficult to understand only by searching the literature. This video shows our technique for the supercharge end-to-side AIN to ulnar motor nerve transfer in patients with ulnar neuropathy.
The cubital tunnel is opened, and the ulnar nerve is identified. Proximal neurolysis of the ulnar nerve is performed by incising the fascia from the medial head of the triceps to the medial intermuscular septum. A 4-cm length of the medial intermuscular septum is excised just proximal to the medial humeral epicondyle. Distal neurolysis of the ulnar nerve is performed by opening the rest of the cubital tunnel, which includes division of the band between the two heads of the flexor carpi ulnaris (FCU) and continuation distally to divide the fascia of the FCU. The flexor-pronator origin is identified, and the fascia overlying the muscle is incised in half along its obliquity. A perpendicular incision is made to connect the fascia-splitting incision with the incision dividing the leading edge of the FCU to create a distal fascial flap. A second perpendicular incision is made to connect the initial fascia-splitting incision with the free proximal border of the flexor-pronator muscle origin to create a proximal flap. The flexor-pronator muscle is then dissected from the fascial edges, which are then sharply excised. The fascial septum separating the pronator teres from the FCU is then excised. The ulnar nerve is transposed, with no tension proximally or distally. The fascial flaps are sutured very loosely with the use of horizontal mattress sutures.
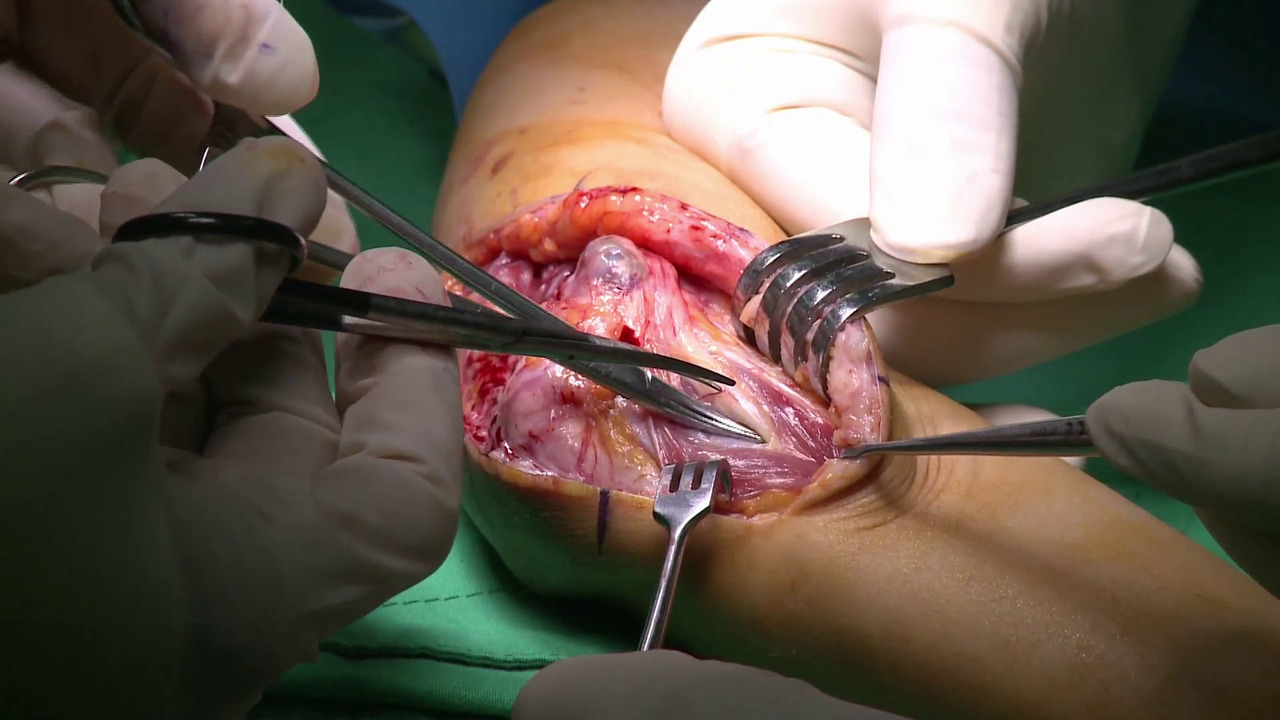
An incision is made ulnar to the thenar crease across the wrist and proximal across the distal forearm. The ulnar nerve and the dorsal sensory branch are exposed in the distal forearm. The ulnar nerve is followed distally, and the thickened antebrachial fascia is released. The Guyon canal is released, and the deep motor branch is decompressed by dividing the tendinous leading edge of the hypothenar muscles. To find the AIN, all the flexor muscles are retracted radially to reveal the pronator quadratus muscle. At the proximal edge of the pronator quadratus, the AIN is identified. The AIN is then traced through the pronator quadratus musculature, transected, and mobilized toward the ulnar nerve for transfer. The motor component is identified between the main sensory component and the dorsal cutaneous branch via interfascicular neurolysis. A perineurial window is made in the motor component, and the coaptation is completed with the use of circumferential sutures.