Modified McLaughlin Procedure for a Chronic, Locked Posterior Shoulder Dislocation
Background
Posterior shoulder dislocations are relatively rare, accounting for less than 5% of all shoulder dislocations. One in every four acute posterior shoulder dislocations is missed on initial presentation. Locked posterior shoulder dislocations are a subset of shoulder dislocations that do not reduce spontaneously because of an engaging reverse Hill-Sachs defect on the posterior glenoid rim. Therefore, surgical management via open reduction and additional stabilization is necessary. Patients without considerable glenohumeral arthritis can be treated via the modified McLaughlin procedure, which involves transfer of the lesser tuberosity with the attached subscapularis into the reverse Hill-Sachs defect.
Purpose
This video demonstrates the modified McLaughlin procedure for the management of a locked, chronic posterior glenohumeral dislocation in a patient with delayed presentation.
Methods
The anatomy of, classification of, diagnosis of, and treatment options for posterior shoulder dislocations are reviewed. The case presentation of a 39-year-old man with epilepsy and one prior shoulder dislocation in the setting of a seizure who presented 7 months after a second shoulder dislocation is reviewed. The patient had a locked posterior shoulder dislocation and a large reverse Hill-Sachs lesion with a deficient posterior labrum. After a thorough discussion of the risks, advantages, and prognosis, the patient elected to proceed with open reduction and the modified McLaughlin procedure.
Results
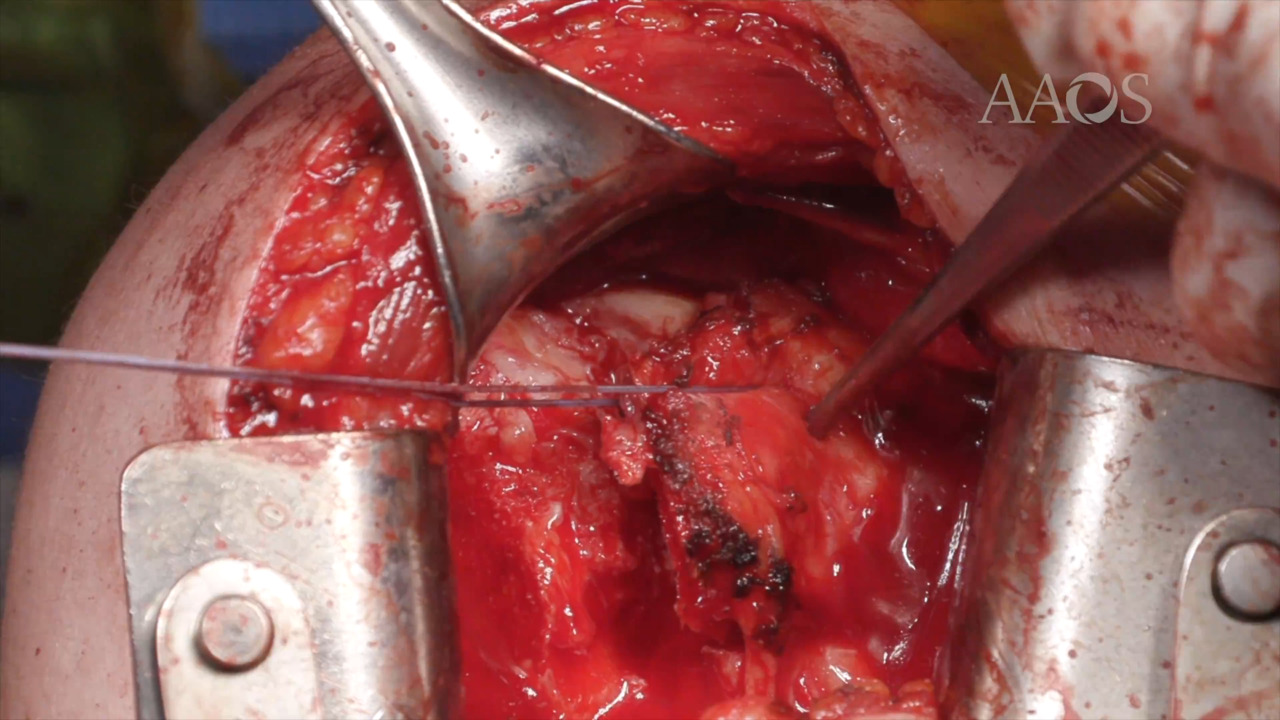
The patient's glenohumeral joint was successfully reduced via open reduction under general anesthesia. Intraoperatively, a 2.5- × 3.5-cm reverse Hill-Sachs defect on the anterior portion of the humeral head was noted to re-engage the posterior glenoid rim with internal rotation. The modified McLaughlin procedure was performed. After decortication of the humeral defect, the osteotomized lesser tuberosity was inserted into the defect. Two double-loaded suture anchors were used to attain transosseous-equivalent double-row fixation of the lesser tuberosity with an anti-rip suture. For supplemental fixation, a 4-mm cancellous screw with a washer was inserted through the lesser tuberosity and into the humeral head. At 3 months postoperatively, the patient had concentric reduction of the glenohumeral joint and maximal range of motion improvements and was progressing through strength training in physical therapy.
Conclusion
A high index of suspicion for a posterior shoulder dislocation must be maintained. Chronic, locked posterior shoulder dislocations almost always necessitate open reduction, with additional procedures indicated based on the size and location of the reverse Hill-Sachs lesion. The modified McLaughlin procedure effectively restores glenohumeral joint stability, with good short-term and midterm range of motion and clinical improvements.