Remnant-Preserving Posterior Cruciate Ligament Reconstruction Using a Posterior Transseptal Portal with Posterior Cruciate Ligament Fovea Landmark
This video discusses remnant-preserving posterior cruciate ligament (PCL) reconstruction using a posterior transseptal portal with the PCL fovea landmark technique.
Typically, the tibial tunneling method is performed with the use of C-arm fluoroscopic guidance during PCL surgery; however, several shortcomings are associated with this method, including influence by natural tibial rotation, hindrance by overlapping anatomic structures, and risk of contamination and radiation exposure. The PCL fovea is the characteristic landmark about the PCL insertion. The PCL inserts at 7 mm anterior from the posterior margin of the PCL fovea in the sagittal plane and at the center of the PCL fovea in the coronal plane.
The fovea landmark technique is used to determine the location of the tibial tunnel without using fluoroscopy. To determine the tunnel position, the medial, lateral, and posterior margins of the PCL fovea is palpated, and the tunnel is made 7 mm anterior to the posterior margin. Given the posterior stress of the graft in the tunnel, the femoral tunnel is made at the eccentric location.
The case presentation of a 48-year-old man with right knee pain and instability is reviewed. On physical examination, the patient had a positive posterior drawer test, posterolateral drawer test, and dial test, and stepping loss was observed.
An outside-in technique was performed on the femoral side, and retro-reaming with the use of a retrograde cutter was performed on the tibial side. A double-stranded tibialis allograft was used. A biocomposite interference screw and post-tie were used for fixation on the femoral side, and an adjustable-loop device and suture tie were used for fixation on the tibial side.
In the patient in this video, anterior cruciate ligament pseudolaxity, abnormal contact, and the drive-through sign were observed on routine arthroscopic examination. The posterior compartment was pressed from outside, and a spinal needle, a No. 11 blade, and a shaver were introduced into the posteromedial compartment. A switching stick was inserted into the posteromedial portal for later insertion of the arthroscope. Then, the arthroscope was shifted to the anteromedial portal and passed to the posterolateral compartment, and the posterolateral portal was established via the same technique as the posteromedial portal. With the surgeon viewing from the posteromedial portal, the posterior septum was pushed with the use of a shaver tip, and the transseptal portal was made at the central portion of the posterior septum behind the posterior cruciate ligament with the use of the shaver.
Finally, the PCL insertion to the PCL fovea was identified. The medial, lateral, and posterior aspects of the PCL fovea were palpated. After placing the drill guide at a 50° to 55° angle, a guide pin was introduced toward the PCL fovea. Tibial reaming was performed with the use of a retrograde cutter. After tibial tunnel preparation, a passing wire was passed from the tibial tunnel and grasped from inside the joint to exit from the anteromedial portal. The arthroscope was introduced from the anterolateral portal, and a longitudinal skin incision was made along the medial border of the vastus medialis muscle at the level of the superior pole of the patella. After dissection of the soft tissues, the entrance to the tunnel was marked on the medial femoral cortex without removal of the remnant PCL. The tip was positioned 5 mm posterior to the distal border of the articular cartilage of the medial femoral condyle. Outside-in femoral drilling was performed. A shaver was then placed in the femoral tunnel from outside, and the tunnel was shaved and cleared.
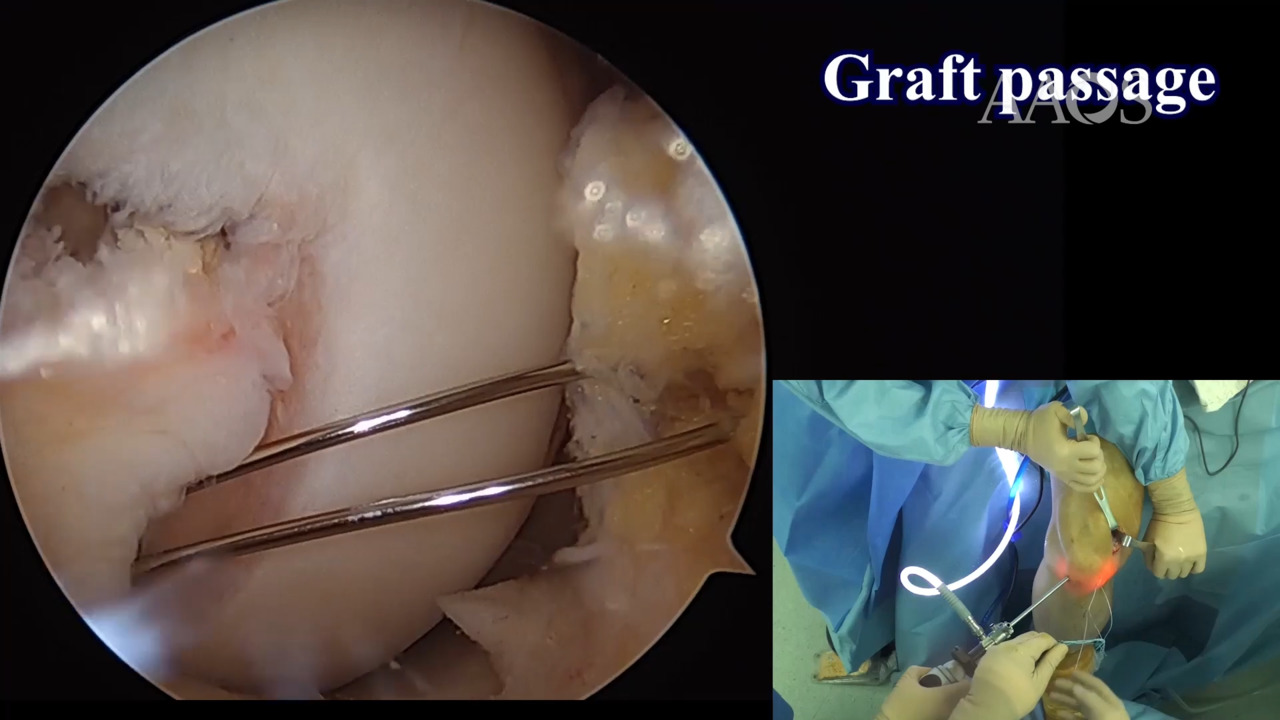
Tibialis anterior allograft, with a diameter of 9 to 10 mm and two strands, usually is used. An adjustable-loop device connected to the tibial side of the graft was passed to the anteromedial portal with the aid of the passing wire. Then, the graft was pulled inside the tibial tunnel until the adjustable-loop device was outside the tunnel. An additional tie-on adjustable-loop device was used to fit it firmly to the cortex of the proximal tibia. A passing wire or suture was then passed from outside-in through the femoral tunnel toward the joint. The passing wire was pulled from the anteromedial portal and was used to pass the graft inside the femoral tunnel. Each strand of the femoral end of the graft should be pulled separately during passage of the graft inside the tunnel. The graft was then tensioned and fixed on the femoral side with the use of a biocomposite interference screw, and fixation was augmented by ligating the excess graft around a spiked washer and screw. Anterior cruciate ligament pseudolaxity, abnormal contact, and the drive-through sign were confirmed to be negative postoperatively.