How to Avoid an Extended Trochanteric Osteotomy: Trochanter-Preserving Osteotomies are Better to Remove Well-Fixed Uncemented or Cemented Stems
Background
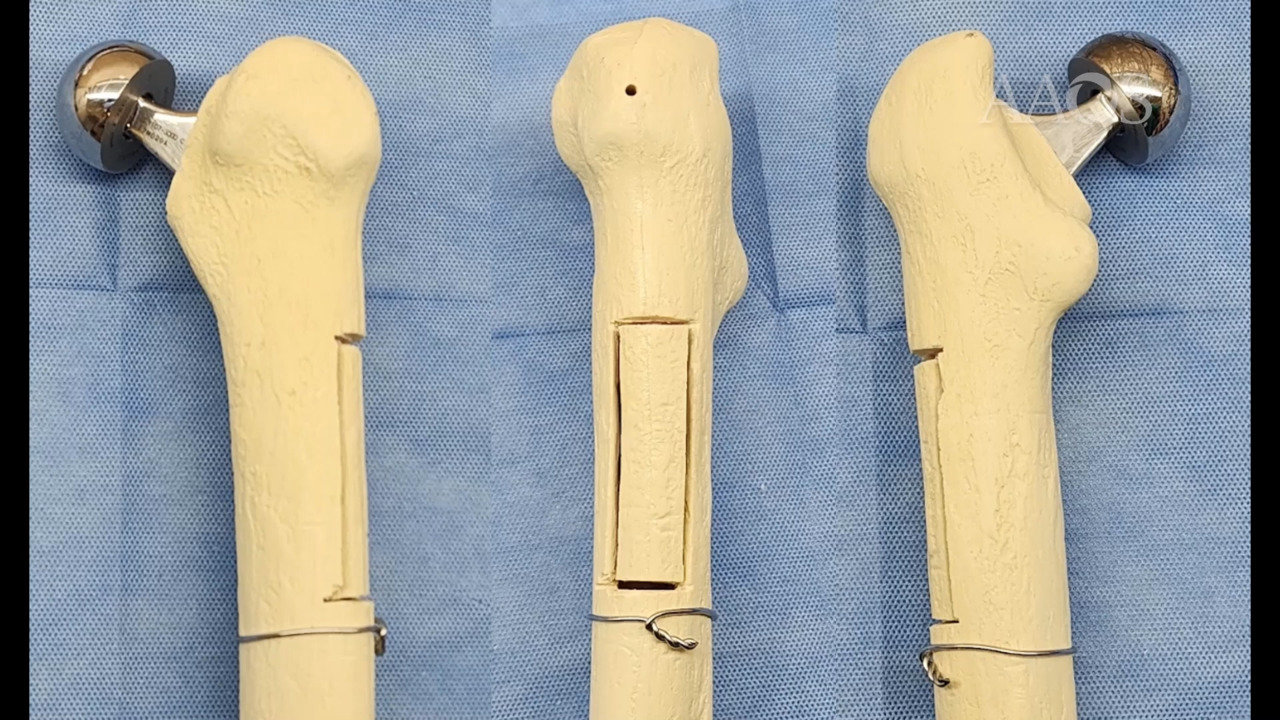
Revision total hip arthroplasty is time-consuming and not without complications, especially if fixed uncemented or well-cemented stems need to be removed. These are complex situations, with a higher risk of complications. Currently, an extended trochanteric osteotomy (ETO) is the preferred treatment option in such cases; however, nonunion has been reported to be as high as 20%, with subsequent risk of a Trendelenburg gait, intraoperative or postoperative femoral fracture, trochanteric migration, and femoral component subsidence. In this scenario, minimally invasive, trochanter-preserving osteotomies are gaining popularity. The goal of this video is to describe the slot osteotomy and a femoral cortical window technique to remove well-fixed femoral components.
Methods
The surgical technique is presented, including tips and tricks, and a case-series of patients who underwent femoral component revision with removal of well-fixed cemented and uncemented stems via a slot osteotomy (ie, limited femorotomy) or a cortical window technique is reviewed. The video sequentially describes preoperative planning, patient positioning, the surgical approach, tips to prevent intraoperative complications, and the postoperative rehabilitation protocol.
Results
Between 2015 and 2022, 647 cases underwent revision total hip arthroplasty with femoral component removal at the authors' center, 57 (8.8%) of which underwent trochanter-preserving osteotomies (20 cortical window techniques and 37 slot osteotomies). Most of the cases (n = 52) showed healing at a mean follow-up of 7.2 ± 3.3 months. One patient in the cortical window group with a diagnosis of a periprosthetic joint infection sustained a postoperative fracture immediately after the second stage (ie, reimplantation), and four patients in the slot osteotomy group underwent intraoperative conversion to an ETO because of fracture propagation without any associated complications. No femoral component loosening or late postoperative periprosthetic fractures were reported at the latest follow-up.
Conclusion
Both trochanter-preserving osteotomies were viable alternatives to remove well-fixed femoral components, avoiding the potential complications associated with an ETO. Although easily extensible and intraoperatively convertible to an ETO if failure occurs (ie, versatile), they help preserve bone stock, with faster rehabilitation, and preserve an unharmed greater trochanter.