Placement of Bilateral Stacked S2-Alar-Iliac Fusion/Fixation Screws With Quad Rods
The lumbosacral junction forms the base of long constructs in spinal surgery and experiences high levels of mechanical strain.Spinal fusion to the sacrum increases sacroiliac joint stress and results in increased sacroiliac joint pain compared with fusions incorporating pelvic fixation. Pelvic fixation increases construct stiffness and fusion rates; however, failure is a potential complication. Martin et al identified a 5% acute pelvic fixation failure rate, which was confirmed in a subsequent multicenter series. Common failure mechanisms include rod or screw breakage, screw loosening, and set-screw dislodgement. Lee et al reported that a higher number of rods crossing the lumbopelvic junction was protective against failure (mean, 3.8 versus 2.9; P = 0.009). Four points of pelvic fixation with four rods spanning the lumbosacral junction has been shown to increase mechanical stability and decrease rod failure and pseudoarthrosis rates at the lumbosacral junction.
A novel sacropelvic fusion/fixation screw designed to prevent these failures recently was approved by the US FDA. The screw has a larger diameter than traditional pelvic screws, a thicker screw neck, a double-lead threaded tip to improve purchase in the ilium, 40° of tulip angulation to aid in rod capture if used in an S2-alar-iliac trajectory, and a more robust set screw with a higher locking torque than traditional pedicle screws. It also has micro- and macro-fenestrations throughout the shank to improve sacroiliac joint fusion rates by promoting bone in-growth and on-growth, with the goal of reducing postoperative sacroiliac joint pain.
This video shows a technique for placement of bilateral stacked sacropelvic fusion/fixation screws in S2-alar-iliac trajectories, with four rods spanning the lumbosacral junction, using intraoperative O-arm based three-dimensional navigation.
The patient is brought to the operating room, and general endotracheal anesthesia is induced. The patient is placed in the prone position on a hinged surgical table, prepared, and draped. Neuromonitoring signals are verified, a timeout is completed, and the patient is administered prophylactic antibiotic agents and tranexamic acid by the anesthesia provider. A posterior midline skin incision is made from the planned cephalad fusion level to the sacrum, and the spine is exposed. A spinous process tracking arc is placed, and three-dimensional images are obtained with the O-arm, which are transferred to the image-guided workstation. Pedicle screws are placed in the thoracic and lumbar spine as necessary, and appropriate positioning is confirmed with two-dimensional and three-dimensional images. A three-dimensional high-density 40° field-of-view scan of the pelvis is obtained before insertion of the S1 pedicle and S2-alar-iliac screws.
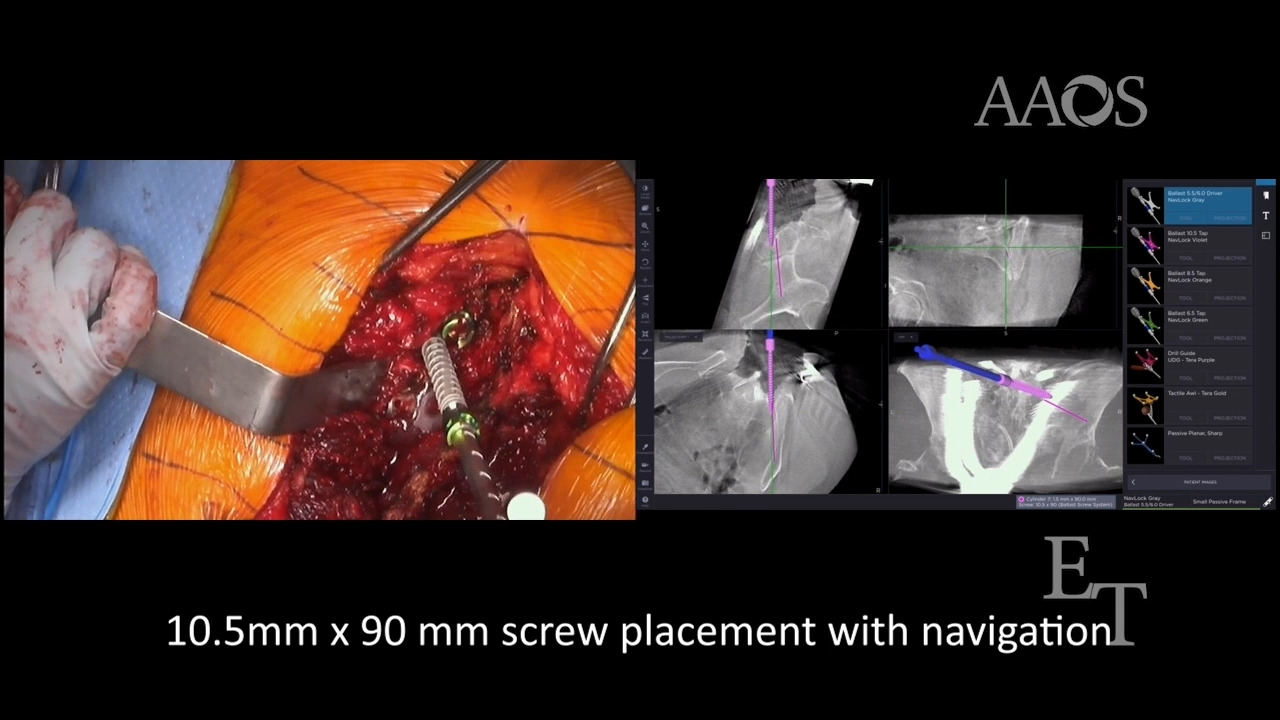
The caudal S2-alar-iliac starting point is identified with the use of a navigated awl, and the trajectory is planned with the image-guided workstation. A mallet is used to take the awl down through the sacrum to the sacroiliac joint but not across it. Next, a tract is created across the sacroiliac joint with the use of a navigated 3.2-mm drill, followed by serial navigated 6.5-, 8.5-, and 10.5-mm taps. Screw length is determined using manual measurements and the image-guided workstation. A 10.5-mm diameter sacropelvic fusion/fixation screw of appropriate length is then placed. This procedure is then repeated for the ipsilateral cephalad S2-alar-iliac screw and the contralateral screws. Two-dimensional and three-dimensional images are obtained to confirm proper positioning.
Additional procedures, such as decompressions and interbody fusions, are performed as necessary. Correcting rods are then placed laterally and seated in the pedicle and cephalad S2-alar-iliac screw heads. Two-dimensional long fluoroscopic images are obtained to verify alignment. Accessory rods are then placed medially and connected to the correcting rods cranially and the caudal S2-alar-iliac screw heads. Three-dimensional, stitched long images are obtained to verify adequate correction, after which torquing of the set screws, posterior element decortication, and fusion are performed. The wound is then irrigated and closed in layers.