A Modified Direct Superior Approach for Total Hip Arthroplasty With MRI Evaluation
Introduction
Although the posterolateral approach for primary total hip arthroplasty (THA) is one of the most used approaches, it is associated with an increased risk of postoperative dislocation compared with other approaches because most of the short external rotators are detached during the conventional posterolateral approach. In 2012, Roger et al described an innovative surgical technique called the direct superior approach (DSA), which is a posterolateral approach that preserves the external obturator and the quadratus femoris muscle. In Asia, a high incidence of secondary hip osteoarthritis results from developmental dysplasia of the hip. This frequently results in severe preoperative hip deformity, limited preoperative range of motion, and leg-length discrepancy that requires lengthening during THA. This video shows a modification of the original DSA technique described by Roger et al to manage these problems.
Surgical Technique
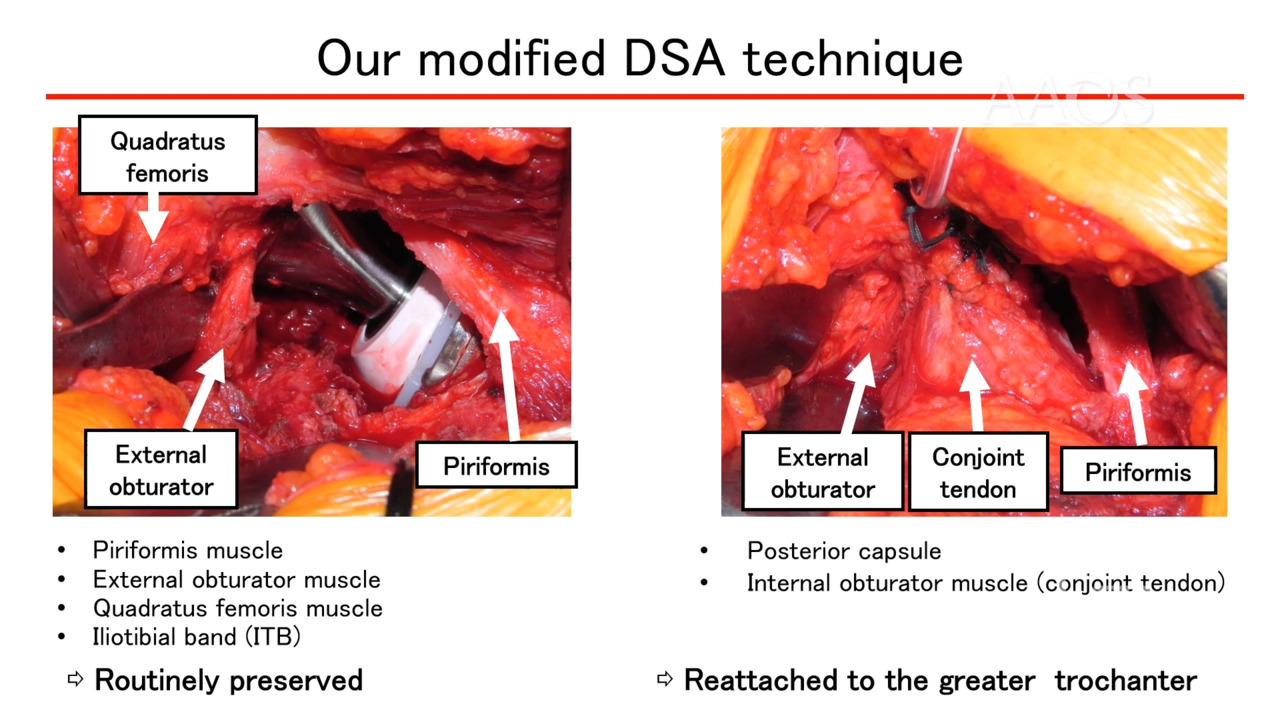
In the modified DSA technique, the piriformis, external obturator, quadratus femoris muscle, and iliotibial band are routinely preserved. The detached internal obturator (conjoint) tendon and the posterior capsule are repaired by reattaching them to the greater trochanter.
In the original DSA, an 8- to 10-cm incision is made at a 45° to 60° oblique angle, starting from the posterior-proximal corner of the greater trochanter. In the modified DSA, a 10-cm skin incision is made at an oblique angle 30° to 45° from the vastus lateralis ridge of the greater trochanter. The original DSA involves the use of a J-shaped capsulotomy, whereas the modified DSA involves the use of an L-shaped capsulotomy. In addition, the modified DSA does not require dedicated retractors intraoperatively. Gentle flexion, internal rotation, adduction, and axial compression are required to dislocate the hip joint.
The original DSA and the modified DSA involve 40° of adduction at 40° of flexion; however, in the modified DSA, internal rotation is limited to 40° to prevent damage to the external obturator muscle intraoperatively. During rasping of the femur, the piriformis muscle needs to be retracted to prevent damaging the muscle. The femur is internally rotated 30°, so the rasping is performed at an angle perpendicular to the ground. The piriformis muscle, external obturator muscle, quadratus femoris muscle, and iliotibial band are routinely preserved in the modified DSA. The posterior capsule and the internal obturator muscle (conjoint tendon) are reattached to the greater trochanter.
Objectives
A study was performed to determine if short external rotators preserved during the modified DSA for THA are well preserved 1 year postoperatively as observed on MRI. Muscle atrophy and fatty degeneration in the short external rotators and the gluteus muscles also were evaluated.
Methods
Between August 2018 and November 2022, the modified DSA for THA was used in 133 cases, of which 81 hips were imaged via MRI 1 year postoperatively. Muscle quality was classified as no atrophy, mild atrophy, or severe atrophy based on the cross-section of the muscle bellies observed on postoperative MRIs. Fatty degeneration was assessed using the Quartile classification system (grade 0, 1, 2, 3, or 4).
Results
The piriformis muscle was successfully preserved in all cases, with no atrophy in 77 hips and mild atrophy in four hips. The external obturator muscle showed no atrophy in 80 hips and mild atrophy in one hip. The internal obturator muscle showed mild atrophy in 33 hips and severe atrophy in 48 hips. The quadratus femoris muscle showed no atrophy in 30 hips, mild atrophy in 17 hips, and severe atrophy in 26 hips. A defect of the quadratus femoris muscle was observed in eight hips preoperatively. The gluteus minimus muscle showed no atrophy in 62 hips, mild atrophy in 17 hips, and severe atrophy in two hips. The gluteus medius muscle showed no atrophy in 65 hips and mild atrophy in 16 hips. Fatty degeneration was observed in the piriformis muscle (grade 0: 78 hips; grade 1: 3 hips), the external obturator muscle (grade 0: 78 hips; grade 1: 1 hip; grade 2: 1 hip; grade 3: 1 hip), the internal obturator muscle (grade 0: 1 hip; grade 1: 22 hips; grade 2: 25 hips; grade 3: 14 hips; grade 4: 19 hips), the quadratus femoris muscle (grade 0: 31 hips; grade 1: 13 hips; grade 2: 9 hips; grade 3: 8 hips; grade 4: 12 hips), the gluteus minimus muscle (grade 0: 7 hips; grade 1: 32 hips; grade 2: 30 hips; grade 3: 8 hips; grade 4: 4 hips), and the gluteus medius muscle (grade 0: 52 hips; grade 1: 24 hips; grade 2: 5 hips).
Conclusions
This is the first study to show the degree of atrophy and fatty degeneration of the hip muscles on the postoperative MRIs of patients who underwent the modified DSA for THA. The procedure revealed good preservation of these short external rotators, except for the internal obturator muscle, which was detached and repaired intraoperatively. Therefore, the modified DSA may improve not only postoperative hip stability but also overall hip function after THA.