Simultaneous Extensor Mechanism Reconstruction and Primary Total Knee Arthroplasty
Background
The number of extensor mechanism injuries have continued to increase over time. The main causes of extensor mechanism injuries include patellar fractures followed by patellar tendon and quadriceps tendon ruptures. In the setting of total knee arthroplasty (TKA), extensor mechanism repair can be achieved with the use of allograft or synthetic mesh.
Purpose
This video provides an overview and discusses a case presentation of a simultaneous extensor mechanism reconstruction and TKA in a patient with a chronic patella fracture with a nonunion.
Methods
The background and surgical treatment options for extensor mechanism reconstruction are presented. The patient is a 58-year-old woman with a history of hypertension, diabetes mellitus, a proximal tibia fracture managed via open reduction and internal fixation, and a patellar fracture managed nonsurgically 22 years ago that resulted in a nonunion. On physical examination, the patient walked with an antalgic gait and had passive range of motion from 5° to 100° but was unable to perform a straight leg raise. Radiographs demonstrated a healed proximal tibia fracture with a lateral plate and screws in place. MRIs of the right knee showed an intact quadriceps amenable to extensor mechanism reconstruction.
Results
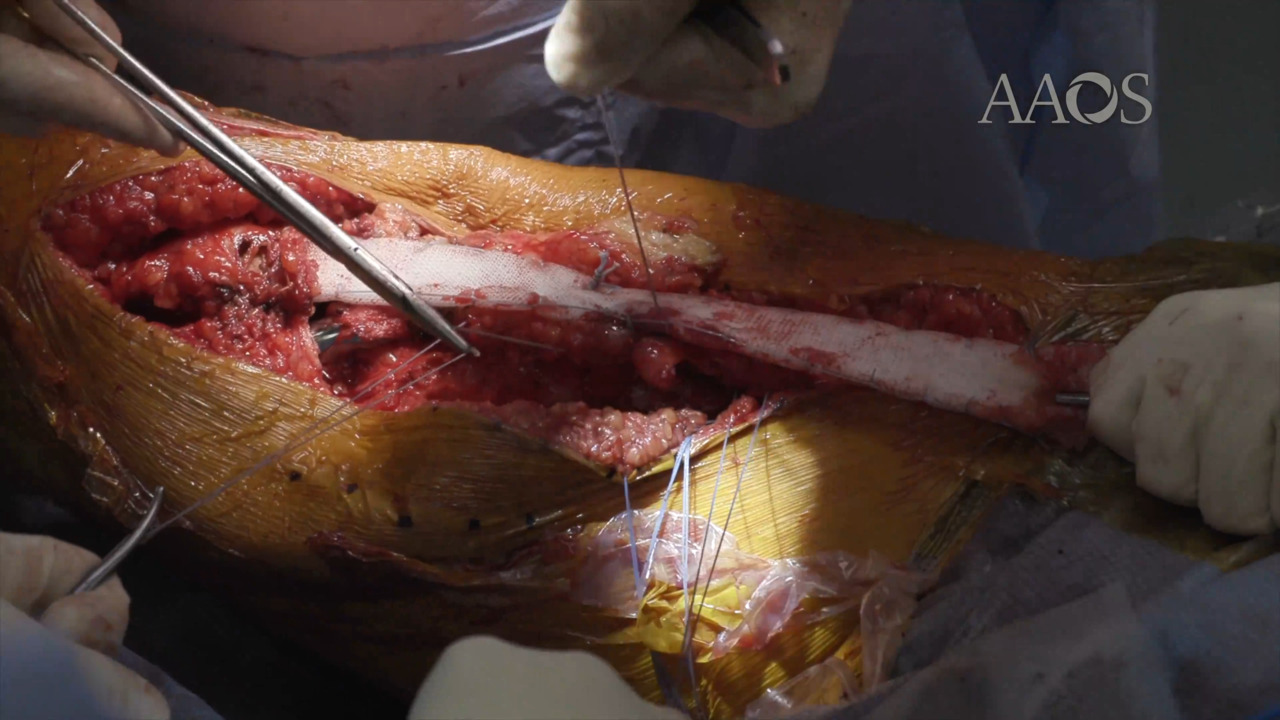
The patient was positioned supine, and prior anterior and lateral incisions were identified. On the back table, the mesh was folded onto itself and locked with the use of suture. The lateral incision was used to remove the proximal screws from the prior fracture fixation construct, which would block the positioning of the TKA tibial implant. The prior anterior incision was used, and a medial parapatellar arthrotomy was made. The quadriceps was mobilized, and the non-united patella was excised. Tibial and femoral bone cuts were made for TKA. During trialing, a nondisplaced lateral femoral condyle fracture was noted and fixed. The tibial canal was burred to allow for placement of the mesh, and the folded mesh and TKA implants were cemented in place. The mesh was sutured to the quadriceps via a pants-over-vest technique, and two drains were placed.
Conclusion
Extensor mechanism disruption in patients undergoing TKA may lead to considerable morbidity and disability. The use of synthetic mesh for extensor mechanism reconstruction can substantially improve patient-reported outcomes and decrease postoperative extensor lag.