Open Bankart Repair: Current Indications and Surgical Technique
Introduction
Traumatic anterior shoulder instability is relatively common in young athletes and the active-duty military population, resulting in capsulolabral injury and loss of constraint by the inferior glenohumeral ligament and thereby substantially increasing the risk of future dislocation. Surgical management of shoulder instability has increasingly shifted toward arthroscopic Bankart repair, which is increasing at a rate of 7.9% annually; however, failure rates associated with arthroscopic Bankart repair may be high, particularly in contact athletes. In addition, in comparative studies, open Bankart repair consistently results in lower recurrence rates and high satisfaction scores. This video presents the modern indications and technique for this procedure.
Indications
Open Bankart repair is indicated in patients with isolated traumatic anterior shoulder instability and patients with subcritical anterior glenoid bone loss (<13.5%). Ideally, the procedure is suited for patients who are involved in contact sports or occupations with high physical demands that may place substantial stress on the repair. Open Bankart repair also is well suited for patients in whom well-performed arthroscopic Bankart repair failed but who do not have substantial progression of glenoid bone loss.
Technique
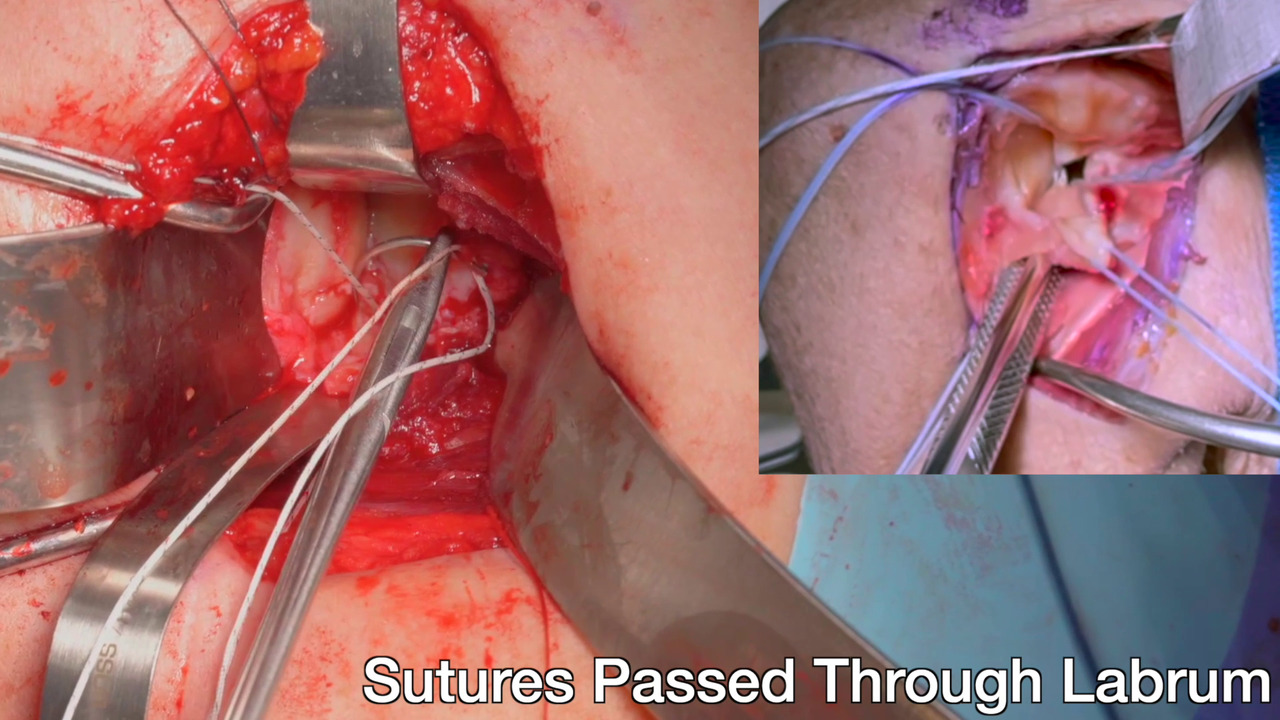
The technique for open Bankart repair is performed with the patient in the beach-chair position and involves the use of standard open shoulder instrumentation and retractors; however, specialized retractors can be used. Before open repair, arthroscopic remplissage may be performed, which helps posteriorize the humeral head for ease of repair and address potentially engaging Hill-Sachs lesions. A deltopectoral interval incision is created, and the conjoint tendon is retracted medially. A transverse incision is made through the subscapularis, which is carefully dissected from the capsule and then tagged at both leaflets for retraction and later repair. A longitudinal incision is then made in the capsule, in line with the anterior glenoid labrum, and extended transversely, in line with the subscapularis split, to form a T-shaped incision that can be tagged for retraction of the superior and inferior leaflets of capsulolabral tissue and later imbrication. The glenoid rim is then prepared, and the capsulolabral leaflets are repaired to the rim in an overlapping fashion, taking care to superiorize the inferior limb and secure the leaflet edges to one another in an overlapping fashion. The subscapularis may then be closed, after which the wound is closed. Rehabilitation is performed under the guidance of a physical therapist, and a sling is used for 6 weeks postoperatively. Return of full motion is expected by 12 weeks postoperatively, and return to sports activity is expected by 6 months postoperatively.
Discussion and Conclusion
Traumatic anterior shoulder instability is a challenging problem for young, high-demand athletes, and surgical repair may yield unsatisfactorily high failure rates. Although arthroscopic Bankart repair is an excellent surgical treatment option for most patients with minimal glenoid bone loss, open Bankart capsulolabral shift may be preferred in patients who participate in high-risk sports/occupations, patients in whom primary procedures failed, and patients with bone loss who do not meet the threshold for bone block procedures. Using a considerate technique with appropriate management of the humeral head and other intra-articular lesions, well-performed open Bankart repair results in reliable restoration of shoulder stability and relatively rapid return to function.