Treatment of Four-Part Proximal Humerus Fractures With a Locking Compression Plate and Fibular Allograft Augmentation
Introduction
Four-part fractures of the proximal humerus are common fractures and generally are managed nonsurgically; however, these fractures are clinically challenging and difficult to manage if displaced or unstable because stable fixation is difficult to attain. Currently, locking compression plating is the most widely used method for the fixation of these fractures in young and elderly patients; however, stable fixation is difficult to attain in patients with osteoporosis. Some studies have reported a high incidence of screw perforation or varus collapse in osteoporotic fractures with severe medial metaphyseal comminution. Good outcomes have been reported with the use of an associated intramedullary fibular allograft. In addition, some biomechanical studies have reported that, under varus bending loads, the augmented construct has an increased initial stiffness and a higher ultimate failure load.
Purpose
This video shows the gross anatomy of the anterior and posterosuperior shoulder, with emphasis on muscle and nerve anatomy. It also demonstrates the fixation of four-part proximal humerus fractures via locking compression plating and fibular graft augmentation in a cadaver model laboratory. In addition, the outcomes of surgical management of this type of fracture via the described technique are reviewed.
Methods
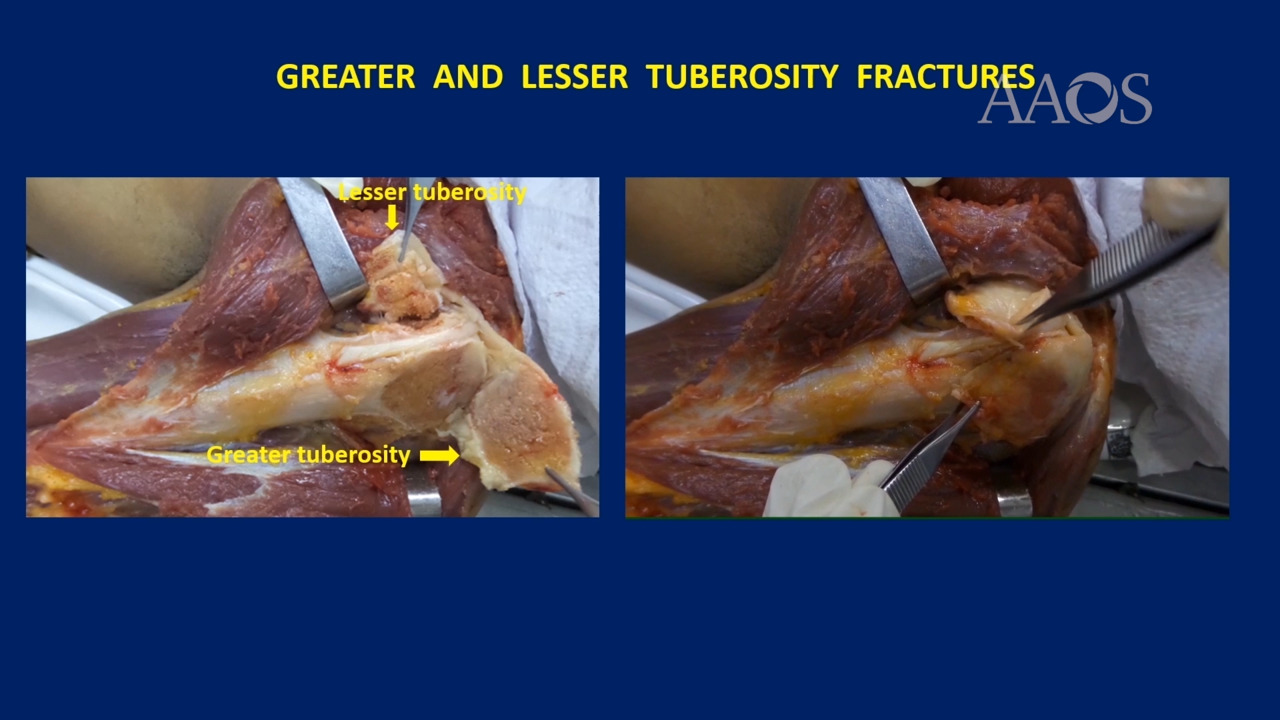
The gross anatomy of the anterior and posterosuperior shoulder and the surgical management of a simulated four-part proximal humerus fracture via locking compression plating and fibular graft augmentation in a cadaver model laboratory are presented. Thirteen patients with a displaced four-part proximal humerus fracture who underwent surgical treatment via locking compression plating and fibular allograft augmentation were retrospectively reviewed. The procedure was performed via a standard deltopectoral approach. A 3.5-mm proximal humeral locking plate was used in all the patients. Nonabsorbable sutures were passed through the junction of the greater tuberosity and the lesser tuberosity and the rotator cuff to promote mobilization and reduce fragmented tuberosities. After reduction of the humeral head and the tuberosities, temporary fixation was attained with the use of one or two Kirschner wires. A locking compression plate was placed 5 to 10 mm lateral to the bicipital groove and 15 to 20 mm inferior to the vertex of the humeral head. The frozen fibular allograft was shaped to a length of approximately 6 to 8 cm, introduced into the medullary canal of the humerus through the fracture site, and impacted into the subchondral bone of the humeral head in a retrograde fashion. Fixation was then attained with the use of screws, after which a tie-down suture of the rotator cuff to the side holes of the plate was used for tuberosity fixation. Finally, the wound was closed. A shoulder immobilizer was used for 3 to 4 weeks. Passive exercises were initiated on the first postoperative day, and active-assisted range of motion was initiated at 4 weeks postoperatively. Outcomes were assessed at a mean follow-up of 28 months (range, 12 to 48 months) via Disabilities of the Arm, Shoulder and Hand scores; visual analog scale scores for pain; and patient satisfaction scores.
Results
Thirteen patients (six males, seven females) with a mean age of 51.16 years (range, 31 to 70 years; standard deviation [SD]± 12.93 years) were included in the study. All the patients had a displaced four-part proximal humerus fracture. The mean Disabilities of the Arm, Shoulder and Hand score increased 19.9 points (range, 1.9 to 38.3; SD± 13.93), the mean visual analog scale scores for pain increased 1.9 points (range, 0 to 7; SD± 2.46), and the mean patient satisfaction score increased 8.9 points (range, 7 to 10; SD± 1.06) at final follow-up.
Conclusion
Proximal humerus fractures in patients with osteoporosis and in younger patients with a four-part fracture who undergo treatment via locking plate fixation and a fibular allograft are associated with good clinical outcomes.