Pediatric Lateral Extra-articular Tenodesis: A Modified Lemaire Technique
Background
The incidence of anterior cruciate ligament reconstruction (ACLR) in pediatric and adolescent patients is substantially increasing, and many patients have risk factors that predispose them to anterior cruciate ligament re-tear. Lateral extra-articular tenodesis (LET) may be performed in combination with ACLR to reduce the risk of anterior cruciate ligament re-tear. The purpose of this study was to determine the 2-year clinical outcomes of ACLR with soft-tissue quadriceps tendon autograft and LET via a modified Lemaire technique in skeletally immature patients. Patients were indicated for LET if one or more of the following risk factors was present: participation in high-risk competitive sports, such as football, lacrosse, soccer, or basketball; grade 3 pivot-shift test; hyperlaxity (Beighton score >4); knee recurvatum; revision ACLR; contralateral ACLR; or chronic ACL insufficiency.
Methods
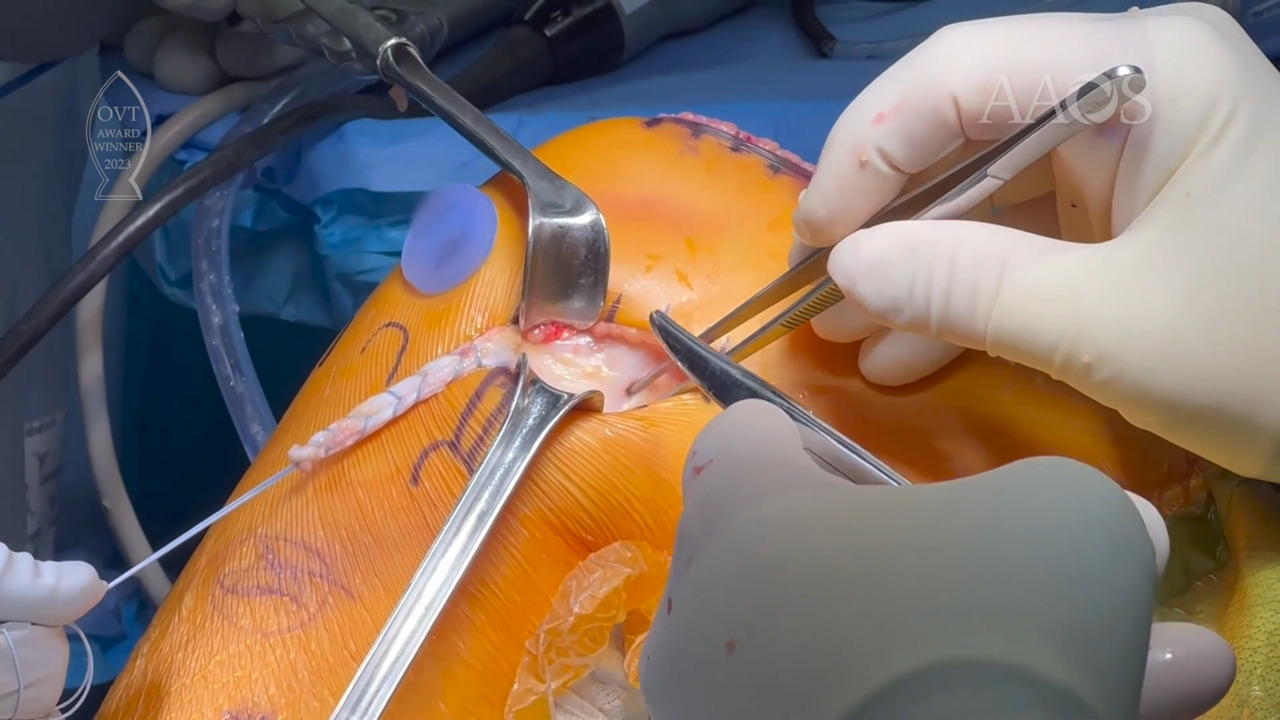
A consecutive series of patients who underwent quadriceps tendon autograft ACLR and LET with a minimum of 2-year follow-up data were analyzed retrospectively. ACLR techniques included all-epiphyseal and complete transphyseal and were indicated based on skeletal age. After completion of ACLR, adjunctive LET was performed. A 6-cm × 1-cm graft from the central third of the distal iliotibial band (ITB) was harvested, preserving the attachment to the Gerdy tubercle. The proximal end of the ITB graft was then passed deep to the lateral collateral ligament from distal to proximal. The ITB graft was then anchored at a location proximal and posterior to the lateral collateral ligament femoral insertion and distal to the distal femoral growth plate. The proximal remnant of the graft was then folded back onto itself and sutured. The ITB donor site was then closed over with the use of high tensile strength nonabsorbable sutures. Outcome measures included return to sports activity; concomitant or subsequent surgical procedures; and multiple patient-reported outcome measures, including Single Assessment Numeric Evaluation, Pediatric International Knee Documentation Committee, and Hospital for Special Surgery Functional Activity Brief Scale scores.
Results
The final cohort included 50 consecutive adolescent patients aged 11 to 16 years (mean, 14.2± 1 years) with a minimum follow-up of 2 years. One patient was lost to follow-up. Of the patients included in the study (n = 49), 98% participated in high-risk competitive sports. Three patients (6%) underwent revision ACLR. Eleven (22%) patients underwent all-epiphyseal ACLR, and 38 (78%) patients underwent complete transphyseal ACLR. Fifteen (31%) patients underwent subsequent surgical procedures. The rate of graft failure was zero. At 2-year follow-up, the median Single Assessment Numeric Evaluation score was 96.5, the median Pediatric International Knee Documentation Committee score was 96.7, and the median Hospital for Special Surgery Functional Activity Brief Scale score was 22.5. The return to sports rate was 100%.
Conclusion
LET during ACLR is safe and should be considered as a concomitant procedure for adolescent patients who are at high risk for a re-tear.