Chronic Distal Biceps Tendon Reconstruction
Objectives
This video presents chronic distal biceps rupture reconstruction via a single-incision approach with semitendinosus allograft and a pectoralis cortical button.
Indications
Indications for the procedure include avulsion of the distal biceps tendon from the radial tuberosity with proximal stump retraction.
Contraindications
Contraindications for the procedure include medical issues precluding surgical management.
Surgical Technique
This video discusses the case presentation an 8-month-old patient with a proximally retracted distal biceps who underwent chronic distal biceps reconstruction via a single-incision approach with an extra-distal humeral incision. In addition, this technique involves the use of a semitendinosus allograft placed via a PulverTaft weave technique and secured with the use of suture tape and No. 2 FiberWire. The reconstructed tendon is reinserted and fixed with the use of a pectoralis cortical button.
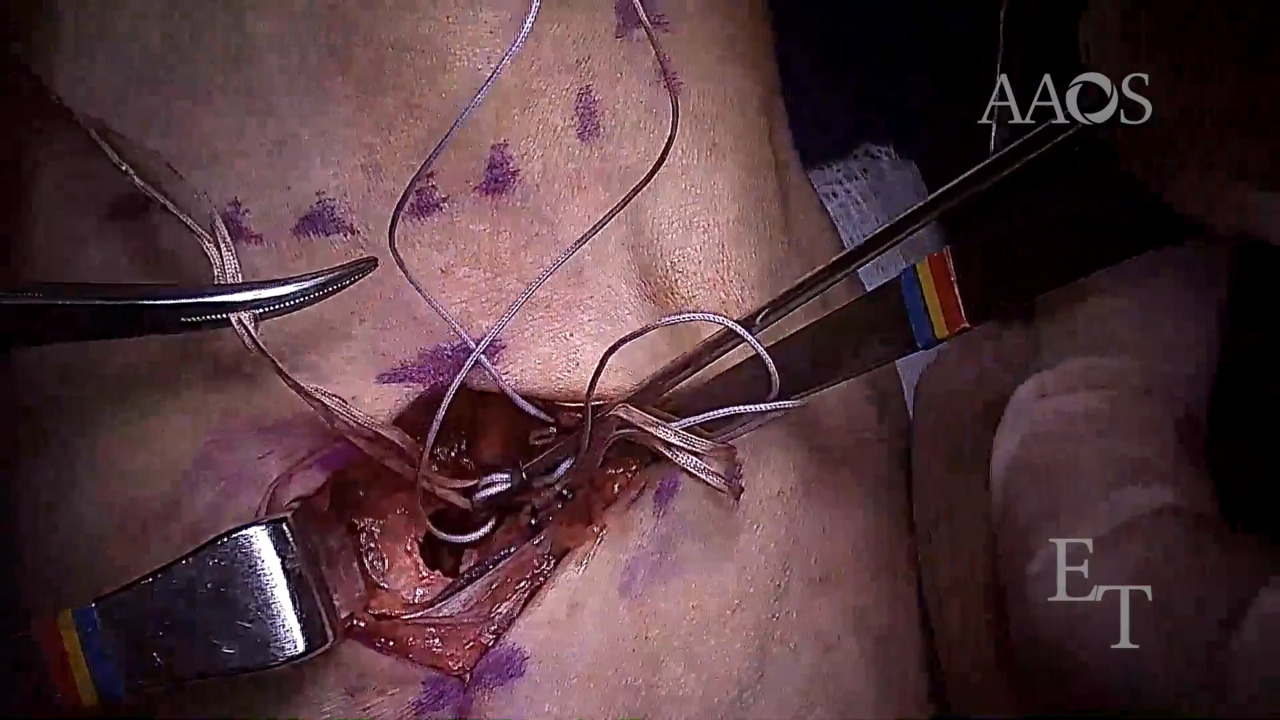
To begin, the forearm in place in supination, and a 4-cm longitudinal incision is made over the medial border of the radial tuberosity. Superficial dissection is carried out to identify and protect the lateral antebrachial nerve. Further dissection is carried down to the radial tuberosity, after which drilling with a guide pin and over drill guide pin is performed for later insertion of the pectoralis cortical button. A secondary longitudinal incision is made medially, proximal to the elbow crease, to locate and retrieve the distal biceps tendon. The distal biceps tendon may be extremely scarred because of the chronicity of the injury; therefore, great care must be taken during dissection. After identification, tendon preparation begins by using a semitendinosus allograft, which is secured to the distal biceps tendon via a PulverTaft weave technique. The two ends of the allograft are fastened together with the use of suture tape and No. 2 FiberWire. After the newly reconstructed tendon is prepared, it is relocated to the anterior proximal forearm. The pectoralis cortical button is prepared by fastening the four limbs of the suture tape and No. 2 FiberWire. After preparation, the anchor device is shuttled through the radial tuberosity osseous tunnel and disengaged. After the button is secured on the cortex, the limbs of the suture tape and No. 2 FiberWire are alternately tensioned. After the tendon is secured, the wound is irrigated and closed. Dressings are applied, and the arm is immobilized.
Postoperative Management
Postoperatively, the patient's arm is placed in a long arm splint in 90° of elbow flexion, with the forearm in neutral. At 1 week postoperatively, the patient's arm is placed in a removable splint. At 2 weeks postoperatively, full elbow flexion in passive and active assisted range of motion is allowed, with extension limited to 60°. At 4 weeks postoperatively, extension is increased to 30°. At 6 weeks postoperatively, full extension and pronation/supination in passive and active range of motion are permitted, with no resisted range of motion permitted. At 12 weeks postoperatively, full weight–bearing and resisted range of motion are permitted.