The Open Capsular Shift Latarjet Procedure for Recurrent Anterior Shoulder Instability
Background
Capsular management is becoming increasingly important during the open Latarjet procedure, especially in preventing postoperative glenohumeral arthritis. The open capsular shift Latarjet procedure consists of a classic Latarjet procedure and a glenoid T-based capsular shift to treat patients with a high risk for recurrent anterior shoulder instability.
Indications
Indications for the open capsular shift Latarjet procedure include patients with humeral and/or glenoid bone loss, patients who participate in professional activities or sports associated with a risk of recurrence, and patients without previous capsular surgery or major capsular deficiency.
Technique
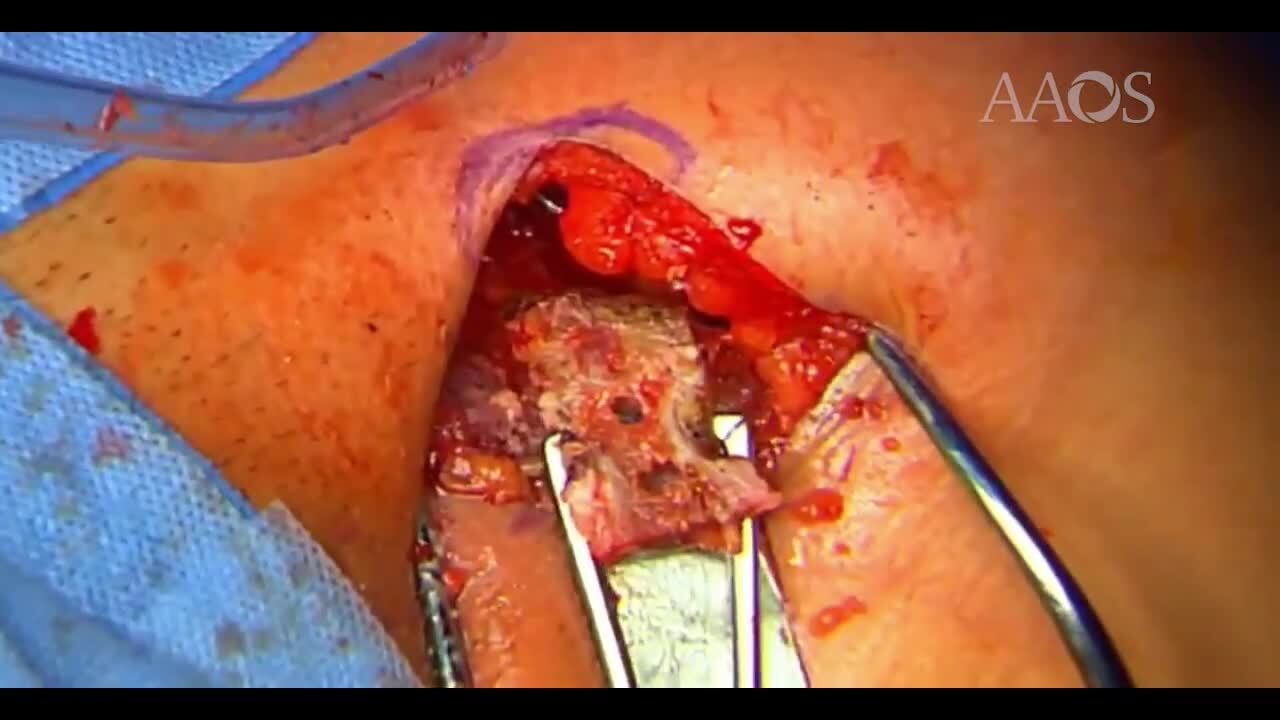
After a classic deltopectoral approach and an osteotomy of the coracoid process, a horizontal split of the subscapularis is performed. Then, a glenoid T-based capsulotomy is performed, and two passing wire suture threads are passed through the inferior flap of the capsule to prepare the capsular shift. A soft, all-suture anchor is inserted at the inferior part of the glenoid medially to the articular surface. The coracoid graft is then positioned with an inferior cancellous screw, made flush with the articular surface, and fixed with the use of a second cancellous screw. A second anchor is placed laterally and superiorly to the coracoid at the anterior scapular neck. The capsular shift is performed via a passing wire technique to suture the capsular flap to both anchors and ensure extra-articular positioning of the coracoid.
Results
Favard reported a low rate of recurrence with no revision surgeries and a considerably lower incidence of osteoarthritis (8.6%) at 10-year follow-up compared with the current literature when suturing the capsule to the coracoid process. Itoigawa reported that suturing the capsule on the coracoid may increase the risk of osteoarthritis because of direct contact between the humeral head and the transferred coracoid; therefore, attachment of the capsule over the glenoid is suggested.
Discussion/Conclusion
With appropriate patient selection, the open capsular shift Latarjet procedure is safe and reliable to treat patients with anterior instability without any specific risks related to the surgical procedure. Capsular repair is an appropriate solution to better restore anatomy and prevent the long-term risk of glenohumeral arthritis.