Bursoscopic Ultrasound-Guided Ossicle Resection for Osgood-Schlatter Disease
Introduction
Osgood-Schlatter disease (OSD) is a painful epiphyseal condition of the tibial tuberosity that was first reported in 1903. OSD frequently affects physically active adolescents. OSD is one of the most common causes of anterior knee pain in this patient population. Approximately 10% of adolescents have OSD. The most accepted theory for the etiology of OSD is repetitive knee extensor mechanism contraction. As a result, avulsions occur at the tibial tuberosity; if the patient continue sports activity, this may result in a separated fragment, leading to nonunion-type pain. OSD is mainly managed nonsurgically, which consists of rest, medications, physical therapy, and proper padding of the tibial tubercle. If symptoms persist after skeletal maturity, surgical management may be indicated. Previous studies have classified surgical techniques as open or endoscopic. Surgical management may involve excision of any mobile ossicles and débridement of the tibial tuberosity. Endoscopic surgery involves a classic arthroscopic approach and a direct bursoscopic approach. The authors of this video used this direct bursoscopic approach. In the direct bursoscopic approach, an arthroscope is inserted into the deep infrapatellar bursa. In comparison to the classic arthroscopic approach, the bursoscopic approach involves the use of more distally placed portals. These portals decrease the risk of damage to the infrapatellar fat pad, the anterior horn of the meniscus, and the intermeniscal ligament. In addition, bursoscopic surgical management facilitates easy removal of ossicles, which are located distal to the deep infrapatellar bursa. A potential disadvantage of bursoscopic surgical management, is the limited working space, especially during débridement of the tibial tuberosity; however, débridement rarely is performed, and the provided space is sufficient for ossicle resection. Endoscopic surgical management, including arthroscopic and bursoscopic approaches, involve the use of intraoperative fluoroscopy because identification of the ossicles covered by bursa is difficult via endoscopy alone. Therefore, the patient is exposed to radiation. The authors of this video use ultrasonography instead of fluoroscopy for ossicle resection. Ultrasonographic-guided ossicle resection is associated with several advantages. First, the use of ultrasonography eliminates radiation exposure. Second, ultrasonography facilitates accurate identification of tiny ossicles, decreasing the risk of remnant ossicles. Compared with the limited view of endoscopy, ultrasonography accurately depicts the surgical field and facilitates identification of small ossicles. In addition, ultrasonography enables visualization of soft tissues, leading to less patellar tendon damage.
Case Presentation
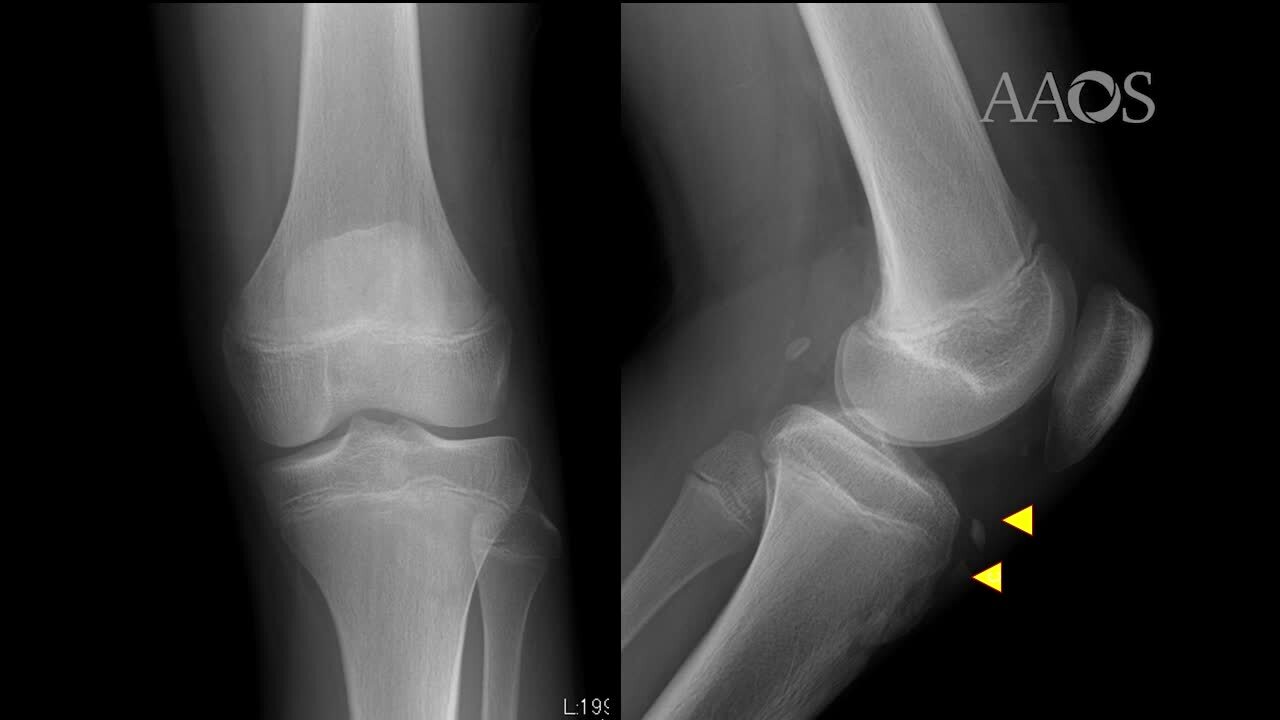
The case presentation of a 14-year-old boy is reviewed. The patient's main symptom was left knee pain. The patient had OSD of the left knee. The patient underwent nonsurgical treatment for 1 year; however, his symptoms became worse. The patient was referred for surgical treatment. Physical examination revealed tenderness of the patellar tendon. Radiographs demonstrated two ossicles, with one ossicle difficult to identify; however, two ossicles were clearly noted on CT scans.
The patient was placed in the supine position on the surgical table, and a thigh tourniquet was applied. The location of the ossicle was confirmed via B-mode ultrasonography. Portals were designated 1 cm away from the medial and lateral edges of the patellar tendon at the level of the ossicle. After the surgical limb was sterilized and draped, a sterile cover was placed over the ultrasonographic probe located on the contralateral side of the patient. This placement allowed the surgeon to visualize the arthroscopic and ultrasonographic monitors simultaneously. Ten milliliters of 1% lidocaine and 10 mL of saline were injected into the deep infrapatellar bursa to mitigate pain and maintain the working space under ultrasonographic guidance using in-plane technique. A 30° arthroscope was inserted into the deep infrapatellar bursa through the lateral portal with the knee in extension. The ossicles were identified via ultrasonography because they are difficult to appreciate via endoscopy. The ossicle was identified by touching it with an arthroscopic probe in the ultrasonographic image. After identification, a 3.5-mm shaver was introduced through the medial portal to resect the bursa around the ossicle. The ossicle was peeled out of the bursa with the use of a radiofrequency device and removed with the use of forceps. After ossicle removal, the area was inspected via ultrasonography to confirm the absence of remnant ossicles, and the incision was closed. Full–weight bearing with full range of motion was permitted immediately postoperatively. Jogging was permitted 2 weeks postoperatively, and strenuous activity was permitted 6 weeks postoperatively.
Conclusion
The bursoscopic approach decreases the risk of damage to the fat pad, meniscus, and ligament. Ultrasonographic-guided ossicle resection is a viable treatment option for OSD because it eliminates radiation exposure and decreases the risk of missed ossicles.