Botulinum Toxin Injection for Digital Ischemia
Introduction
This video shows a technique for botulinum toxin injection for the management of digital ischemia. This technique is off-label use of botulinum toxin.
Indications
Botulinum injection is used to manage vasospastic and occlusive disease of the hand, often in patients with Raynaud disease or Raynaud phenomenon. It also is indicated for impending tissue loss or rest pain refractory to conventional medications.
Inpatient Versus Outpatient
The inpatient setting is for the management of acute ischemic events and as a bridge from intravenous to eventual oral therapy. Outpatient treatment addresses chronic disease, offering adjunctive management alongside oral medications to ameliorate vasospasm and avoid the morbidity associated with surgical sympathectomy. Outpatient insurance authorization often is a lengthy process. This must be considered in patients with impending tissue loss.
Patient Case
This video reviews the case presentation of a patient with scleroderma and Raynaud phenomenon who had notable digital ulceration and trophic skin changes. The patient was admitted for acute exacerbation of bilateral digital ischemia. Treatment was initiated with intravenous phentolamine and alprostadil, which improved the patient's symptoms of rest pain. Botulinum injection was used as an adjunct to bridge from inpatient intravenous medication to eventual outpatient therapy.
Equipment
Surgeons should ensure the necessary equipment is available.
How to Draw Up
The key preparatory step involves ensuring proper dilution of the botulinum solution with normal saline. Various dilution options to create the desired botulinum toxin concentration exist in the literature. These can be titrated based on surgeon discretion, depending on injection location and tissue compliance. The preference of the authors of this video is a concentration of 10 units per cc. The procedure is demonstrated in the video. 10 cc of normal saline is drawn into a 10-cc syringe. This is injected into the 100-unit Botulinum vial, creating a concentration of 10 units per cc. The combined solution is then drawn up and ready to be injected.
Injection Locations
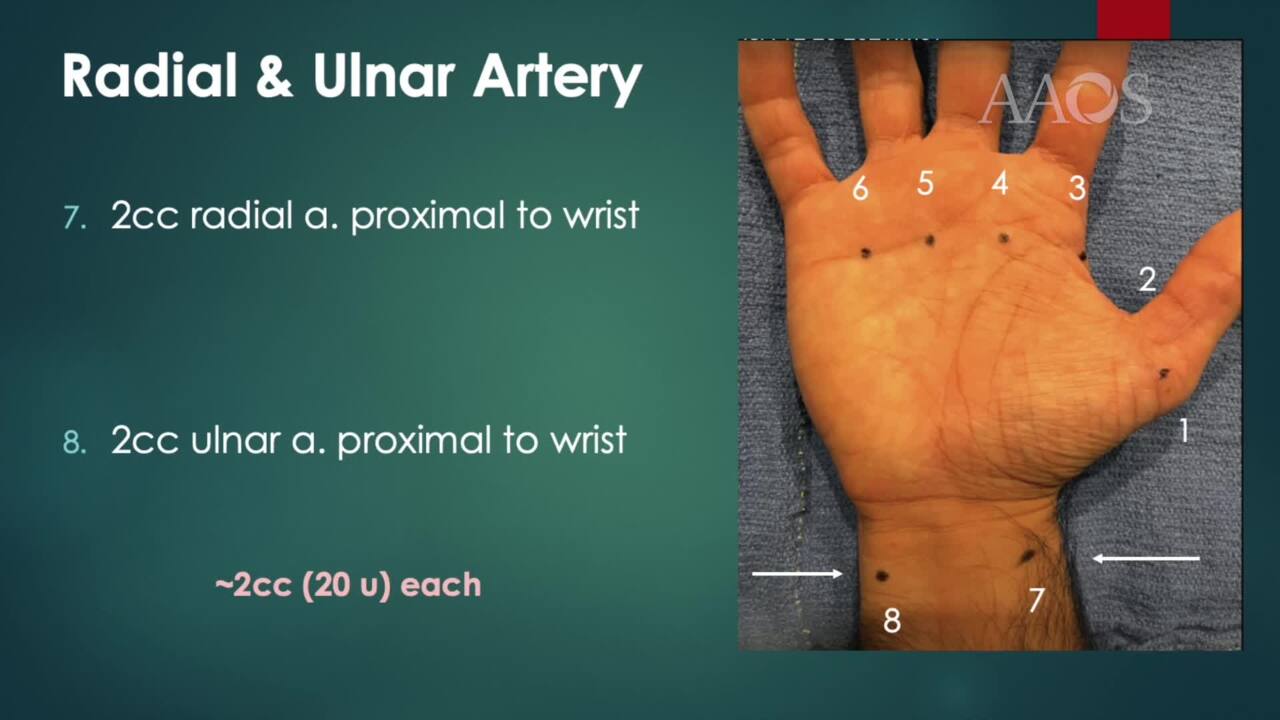
Some studies advocate selective injection of only the involved digits, whereas other studies recommend complete hand management, even in patients with localized disease. The practice of the authors of this video is complete hand management, with eight injection sites for inpatient acute ischemia. A photo with superimposed digital vasculature demonstrates the locations of the eight injection sites relative to arterial supply. We use six injection sites on the volar hand to manage the base of the thumb and the common digital arteries. 1 cc, or 10 units, is injected at each site. An additional 2 cc, or 20 units, is injected over the radial and ulnar arteries proximal to the wrist. The key distinction is the radial and ulnar arteries receive 2 cc each, whereas the six volar hand sites receive 1 cc each. After sterile preparation, the thumb is injected, progressing ulnarly across the palm; however, the injection order does not matter. Webspace injections are administered proximal to the A1 pulley. Surgeons should penetrate deep to the palmar fascia before injecting to ensure the botulinum reaches the arteries. Most patients tolerate the injection; however, it may be quite painful. Topical lidocaine or a lidocaine wrist block may be considered before injection. Surgeons should avoid ethyl chloride for skin anesthesia because it may exacerbate symptoms. Radial and ulnar arteries receive 2 cc each. Surgeons should determine if a pulse is present and aspirate before injection.