Modified Broström Procedure With Suture Tape Augmentation: Surgical Technique
Background
Chronic lateral ankle instability occurs in 20% to 30% of patients who sustain an ankle sprain, and one in three patients forgo or decrease activity after the modified Broström procedure, which is a weaker construct than the native ligament. Recovery after the modified Broström procedure is problematic, often requiring 3 to 6 weeks of cast immobilization and 3 to 6 months before full recovery. In addition, early rehabilitation in patients undergoing the modified Broström procedure have demonstrated increased laxity and morbidity compared with delayed rehabilitation.
Preoperative Planning
The senior author prefers the InternalBrace (Arthrex) device system for suture-tape augmentation (STA), using 3.5-mm BioComposite SwiveLock (Arthrex) to anchor fixation in the talus and a 4.75-mm BioComposite SwiveLock for fibular fixation. No re-draping is performed between arthroscopic and open procedures.
Surgical Technique for the Modified Broström Procedure with STA
Standard ankle arthroscopy Diagnostic arthroscopy is performed to examine all parts of the joint. Surgeons should identify and address pathologic pain generators.
Approach for the modified Broström procedure with STA (landmarks, incision, structures at risk, dissection) A linear incision is made across the distal fibula, approximately 1 cm proximal to the distal terminus, followed by sharp dissection to the inferior extensor retinaculum and the lateral ligament complex. The superficial peroneal nerve is protected during superficial dissection. The incision is extended in a curvilinear fashion to expose and manage peroneal tendon or superior retinacular tears.
Modified Broström procedure The anterior talofibular ligament is isolated along with the periosteum and the joint capsule soft-tissue cuff in conjunction with the inferior extensor retinaculum. Two 2.4-mm BioComposite SutureTaks (Arthrex) are implanted at the anterolateral aspect of the distal fibula to repair the anterior talofibular ligament, the calcaneofibular ligament, lateral ankle capsule, and extensor retinaculum. Before anchor placement, surgeons should ensure that fibular anatomy will accommodate a 4.75-mm SwiveLock with FiberWire centrally. FiberWire from the BioSutureTak anchor is passed through the soft-tissue cuff from the articular side to the extra-articular side.
Talar anchor A 2.7-mm drill bit with a guide sleeve is placed within the sinus tarsi 2 cm from the tip of the lateral talar process, immediately adjacent to the articular surface at the talar lateral ridge (angled 45° cephalad and medial). The drill is angled 45° cephalad and medial to avoid joint violation. The guide handle should approximate the 7:30-o'clock position (left foot). A 4.75-mm SwiveLock anchor loaded with FiberTape is tapped into the talar hole until the driver's laser line appears, indicating the screw is flush. Alignment the instrument laser lines indicate the screw is 2 mm countersunk.
Complete modified Broström procedure The posterior drawer maneuver is performed with the ankle in a neutral position before securing the anterior talofibular ligament and the capsular sleeve to the fibula.
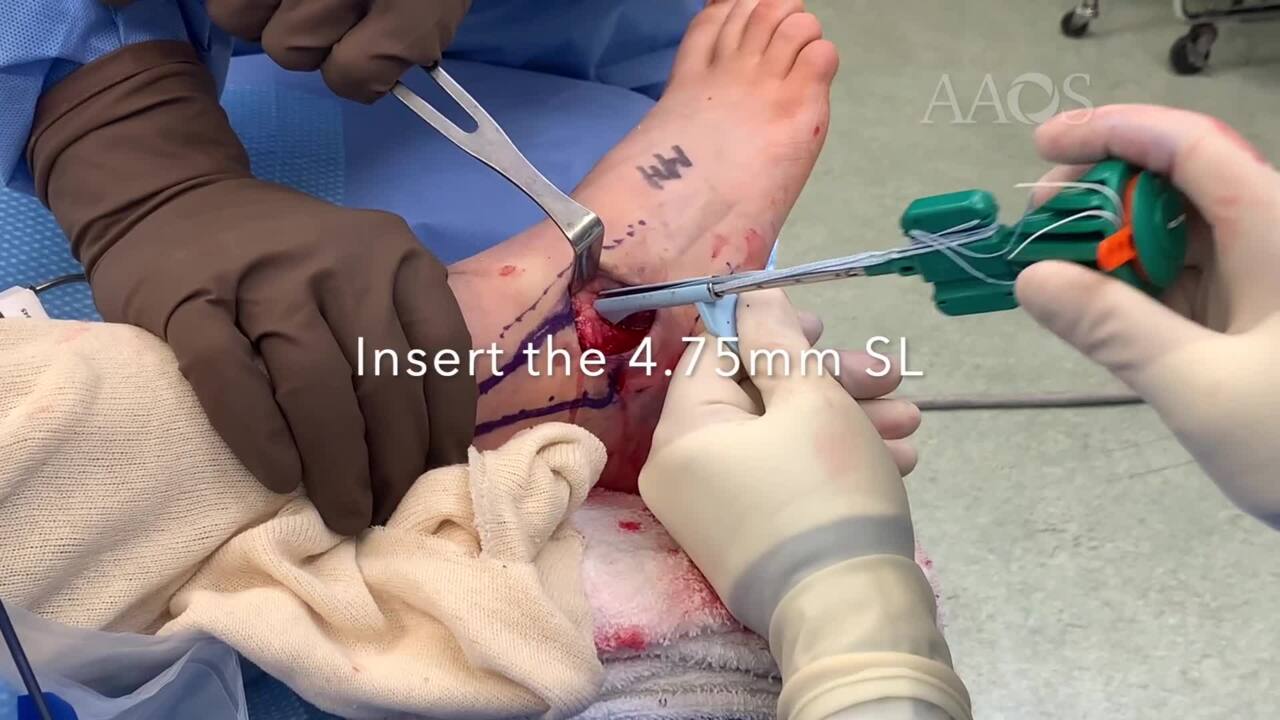
Fibular anchor The second anchor for STA fixation is placed at the anterolateral fibula. The 3.4-mm drill bit is placed 1.5 cm proximal to the distal fibular tip, at the midpoint between all suture anchor implantation sites. A cephalad trajectory is used. The ankle should be neutral in the coronal and sagittal planes for tensioning of the 3.5-mm SwiveLock anchor.
FiberTape management
Excess suture should be excised after final anchor placement. Residual suture may be placed in the inferior extensor retinaculum and approximated proximally with the fibular periosteum or the capsule.
Potential complications
The modified Broström procedure with STA construct The senior author of this video has a predilection for talar anchor placement before fibular anchor placement because biomechanical evidence found the construct to be strongest. Therefore, the 4.75-mm SwiveLock is placed in the talus and followed by the 3.5-mm SwiveLock in the fibula.
Suture mismanagement Suture management is critical, and differentiation of the proximal and distal sutures should be monitored carefully. After inserting both 2.4-mm BioSutureTak anchors in the distal fibula, the superior anchor suture is maintained superior to the FiberTape and the inferior anchor suture is maintained inferior with a 15-mm suture limb spread.
Recurrent or recalcitrant instability Recurrent or recalcitrant instability highlights the importance of patient selection and management of concomitant pathology during the index procedure. Surgeons may consider excluding patients with generalized ligamentous laxity, neuropathy, or occult boney/tendon/chondral pathology.
Postoperative Management
On the day of surgery, the patient's leg is placed in a splint or a controlled ankle motion boot with or without ice. Postoperative days two to three involve a wound check in the clinic and a transition to weight bearing as tolerated in a controlled ankle motion boot. Daily active dorsiflexion/plantar flexion is encouraged, and patients are counseled to avoid inversion. At 3 weeks postoperatively, the patient is transitioned to an ankle stabilizing orthosis brace and a normal shoe. Formal physical therapy is initiated. At 6 weeks postoperatively, sport-specific training is initiated, and running on a treadmill is allowed. At 10 to 12 weeks postoperatively, patients can return to play.
Return to Sports Activity
The most important indicators for return to sports activity are joint stability, muscle strength, and full range of motion. Few studies have reported on return to sports activity as an outcome metric in patients with chronic lateral ankle instability. Patients are allowed to return to play 10 to 12 weeks postoperatively.
Published Outcomes:
Laboratory data demonstrate that STA conferred superior construct strength, and early clinical data, including level I through IV evidence, portend favorable trends for the modified Broström procedure with STA.
Preliminary data indicated STA is a safe and durable supplement to the modified Broström procedure, facilitating accelerated rehabilitation protocols and return to activity without concomitant increased morbidity risks. Conversely, early rehabilitation in patients undergoing the modified Broström procedure is associated with an increased risk of morbidity compared with delayed rehabilitation.
The modified Broström procedure with STA is associated with accelerated recovery and return to activity, with decreased postoperative pain, speculated to be secondary to increased construct strength. Future studies may reveal STA to be protective against future injury.