Complex Primary Total Hip Arthroplasty in Cases With Previous Proximal Femoral Devices: How to Avoid Old Implant Removal and Revision Stems
Background
Primary total hip arthroplasty (THA) in patients with hip osteoarthritis results in excellent long-term outcomes with regard to pain reduction and improved function and quality of life. The most frequent scenario is an older patient with hip osteoarthritis but no other associated hip pathology; however, some patients with developmental dysplasia of the hip or corrective osteotomies from a history of trauma have femoral plates or screws from previous treatment. These patient populations have failure rates ranging from 18% to 30% after 10 years and 60% after 15 years, and conversion to primary THA usually is necessary. Previous proximal femur devices create technical difficulties during primary THA. Usually, these patients also have abnormal proximal femur anatomy and sclerotic metaphyseal bone that poses a challenge in femoral canal preparation, increasing the risk of complications, such as intraoperative fractures and component malpositioning.
Methods
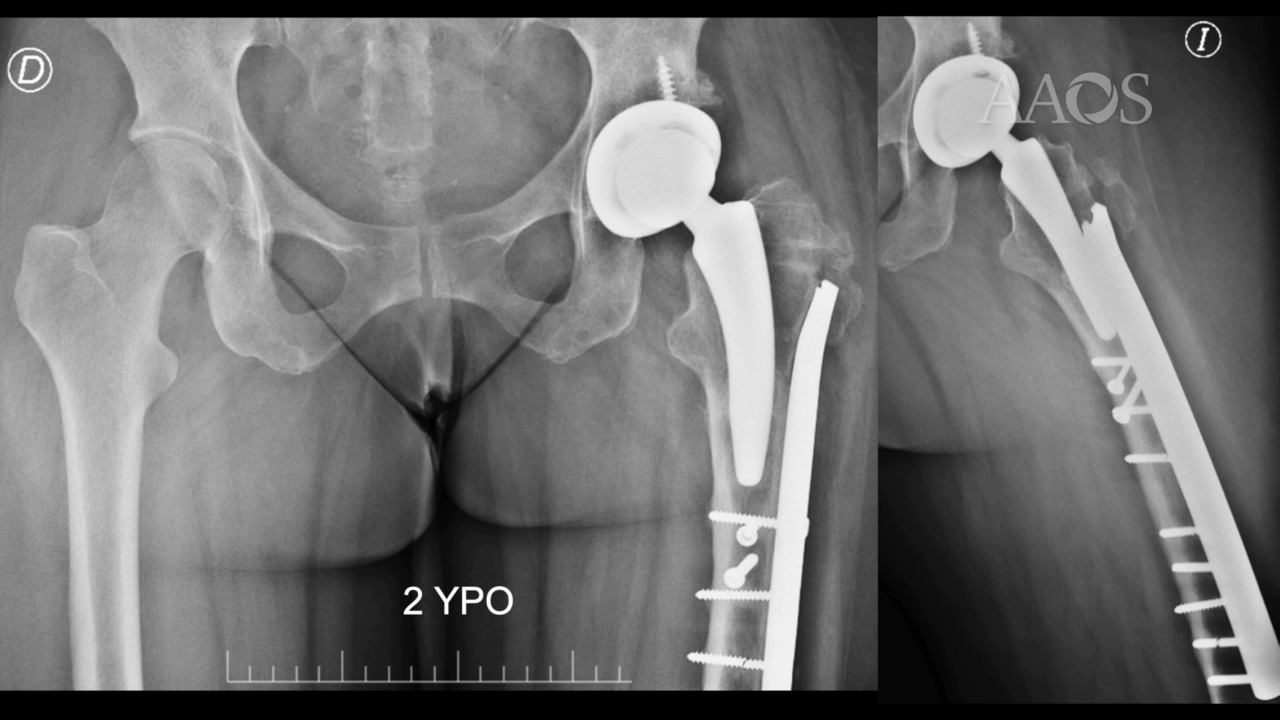
This video presents complex situations in patients with previous proximal femur plates and screws who underwent different types of primary THA via partial or no implant removal, corrective osteotomy, and a distally fixed revision stem. In addition, preoperative planning, patient positioning, surgical approach, tips and tricks to prevent intraoperative complications, and postoperative rehabilitation protocols are described.
Results
No intraoperative or postoperative complications, such as dislocation, infection, or revision of the femoral component for any cause were reported in a series of ten cases. The mean postoperative minimal disease activity score was 16 points (range, 14 to 18).
Conclusion
Primary THA is possible in many patients with previous proximal femur devices without the need for implant removal. Alternative treatment options range from conventional cemented or uncemented stems, to surface arthroplasty, to short stems. The technique is demanding and requires experienced surgeons. If possible, complete implant removal should be avoided, and distal fixed femoral stems should be used to preserve bone stock and decrease costs.