Split Pectoralis Major Transfer for Serratus Paralysis: Changing the Paradigm of Scapular Winging
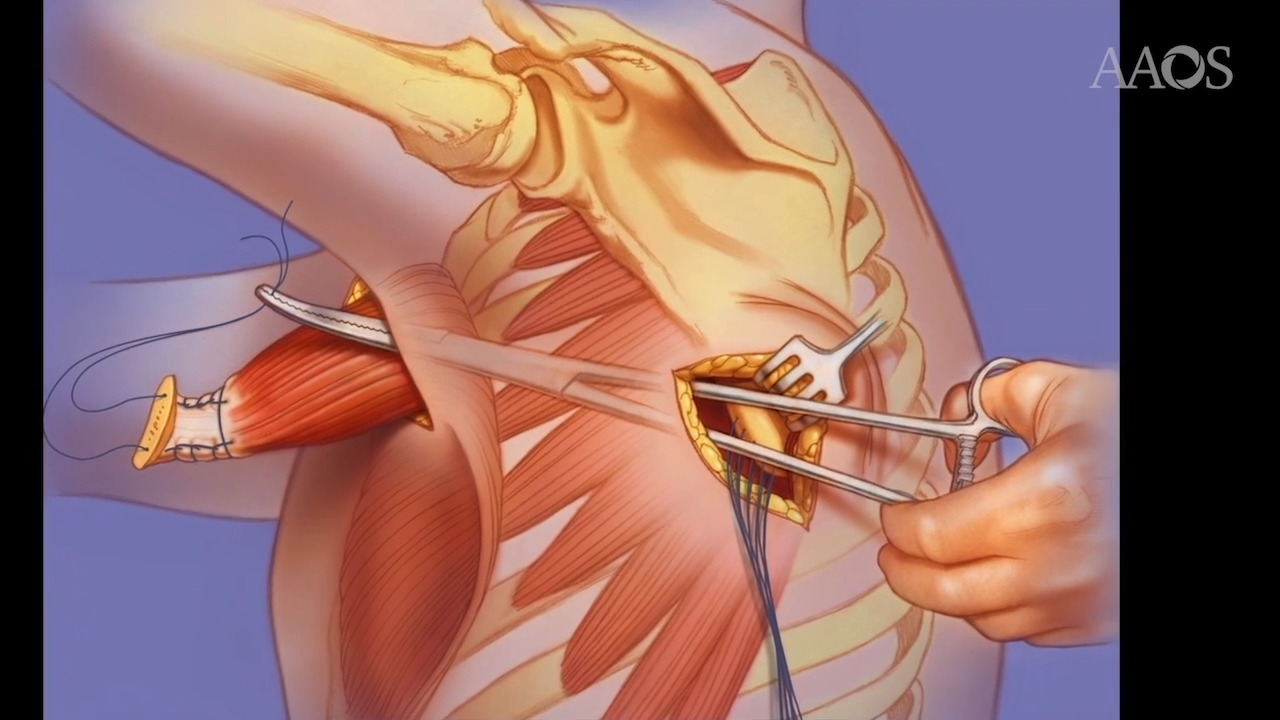
Case Overview: We present the case of a female who experienced right scapular winging and shoulder pain for 1.5 years. Technique: With the patient in the semilateral position, the incision was performed from the anterior axillary fold proximally toward the coracoid to expose the pectoralis major (PM) insertion. The fascial attachment of the proximal part of the tendinous insertion of the PM to the biceps groove was released. The most distal tendinous aspect of the clavicular head was detached from the humerus, then separated from the sternal head medially. The PM tendon was then detached with 5 mm of its bone insertion from the humerus. A #2 Orthocord suture was placed in both the clavicular and the sternal head for later repair. Then the shoulder was placed in flexion, allowing the scapula to protract against the chest wall. The distal part of the scapula was palpated, and a slightly curved incision was made from the distal tip of the scapula medially, 5 cm in length. The SA tendinous insertion was identified, and a #2 Orthocord suture was placed to assist in later mobilization of the scapula and to reinforce the tendon transfer. To expose the posterior aspect of the distal tip of the scapula, the origin of the teres major was partially detached. Multiple #2 Orthocord sutures were placed in transosseous fashion circumferentially around the prepared distal tip of the scapula to be used for the repair of the tendon transfer. The shoulder was then placed in abduction, and a tunnel was created between the anterior and posterior wound. A Carmalt clamp was passed deep to the scapula from the posterior wound, gliding on the chest wall toward the anterior wound. The suture of the sternal head of the PM was placed in the Carmalt clamp to allow passage of the muscle along the chest wall toward the prepared scapula. Once the bone attachment of the sternal head of the pectoralis was retrieved from the posterior wound, the shoulder was placed in flexion, and the raw surface of this bone attachment to the prepared tip of the scapula was repaired. The Krakow sutures were then placed in the sternal head of the PM, and the sutures placed in the tendinous portion of the SA were further passed around the repair site to augment and to reinforce the repair. Once the transfer was accomplished, attention was directed to repair the clavicular head of the PM to its original footprint. Results: In a study by Elhassan and Wagner 2015 in which the outcomes of patients who underwent this transfer with inclusion of the bone insertion were evaluated, it was found that this technique resulted in resolution of winging in most patients and showed significant improvement in shoulder abduction, forward flexion, and pain levels. Summary: Direct transfer of the sternal head of the PM tendon with its bone insertion to the lower pole of the scapula leads to great outcomes in treating patients who have symptomatic scapular winging secondary to chronic SA dysfunction.