A New Minimally Invasive Plate Osteosynthesis Approach for the Humerus: A Farewell to the Radial Nerve
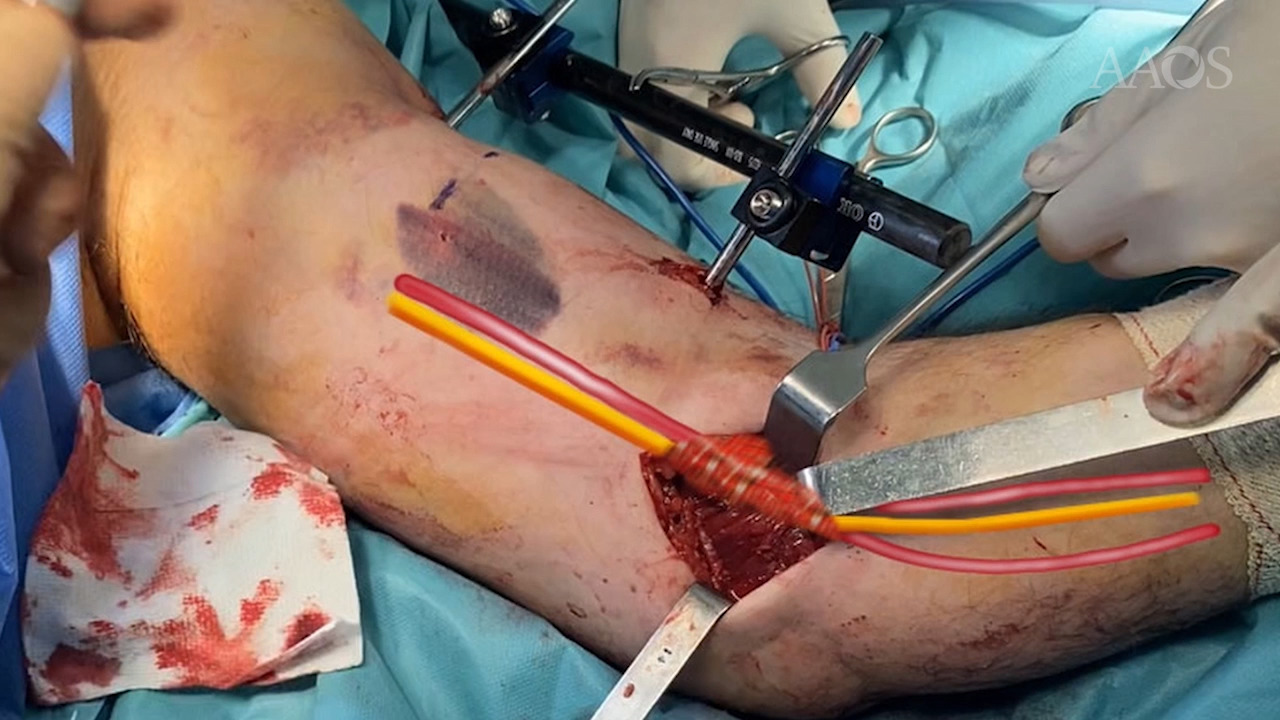
Distal third humeral shaft fractures remain a challenge today. Open surgical approaches for plate fixation are laborious, and a high incidence of iatrogenic radial nerve palsy has been reported. To solve these problems, minimally invasive plate osteosynthesis (MIPO) techniques were described; however, they do not solve the problem of the radial nerve. Posterior MIPO approaches applied to the distal third are very uncomfortable, because the patient has to undergo surgery in the prone position. The radial nerve must be referenced at the proximal incision, which makes surgery laborious and increases the possibility of a transient radial nerve palsy. A distal MIPO Kocher approach has been also described without identifying the nerve. It is in fact a blind radial nerve MIPO technique that causes stress to the surgeon and carries a high risk of radial nerve damage. We describe an anteromedial distal minimally invasive approach in which direct damage to the nerve is fully avoided. The approach is performed through the fibers of the proximal belly of the pronator teres muscle to expose the anterior flat area of the medial epicondyle where the distal part of the plate is assembled. The main advantage is that the nerve cannot be directly damaged. We have used this approach in mid- and mid-distal shaft fractures, but we have excluded patients with open fractures, previous radial nerve palsy, or any other neurovascular injuries. The most frequent mechanisms of injury in the study patients were accidental falls, work, car or motorbike accidents, and periprosthetic and metastatic fractures. Although this technique was originally described for fractures of the distal third, it also can be applied successfully for middle shaft fractures, and sufficient stability is achieved. Surgical Technique Patients underwent surgery in a comfortable supine position with the arm extended to a side table. General anesthetic was used in all cases, and no tourniquet was applied. The elbow was flexed about 30&[deg] to relax the brachialis muscle and to reduce the deformity, especially if an external fixator was not to be used. Although bone reduction can be achieved by manipulation, we recommend a temporary external fixator to maintain reduction during the insertion of the plate. Distal pins of the external temporary fixator must be introduced in radial nerve damage–free zones to avoid radial nerve palsy, which is the real aim of this novel approach. We consider that there are two safe zones for the distal introduction of the pins. The first one is the lateral center of the capitellum and the other one just above the coronoid fossa through a small incision very close to the external border of biceps tendon. First we perform the distal approach. Superficial landmarks to identify the biceps tendon and the medial epicondyle are drawn. The skin incision begins 3 cm proximal to the elbow crease and extended distally for another 3 cm. It is performed halfway between the inner portion of the biceps tendon and the apex of the medial epicondyle. The subcutaneous cellular tissue is dissected. Superficially, the medial antebrachial cutaneous nerve and the basilic vein must be identified and retracted. The ulnar nerve is never identified because it is protected by the medial intermuscular septum and its posterior pathway. The neurovascular bundle runs over the belly of the brachial muscle about 2.5 cm lateral to the muscular incision and can be identified if desired. Posteriorly, the proximal belly of the medial epicondyle muscles is identified. The most important step is to identify the muscular belly of the epicondylar muscles that are protected by their muscular fascia. Fascia must be open for correct identification of the muscular fibers. A muscular incision is made, starting 1 cm lateral to the medial epicondyle and extended distally for another 3 cm through the anatomic direction of the pronator teres muscular fibers. Osteosynthesis of the fracture is performed by using a 10-hole extra-articular elbow locking compression plate. This is an off-label use of the plate; it has to be molded to provide an adequate fix on the anterior medial epicondyle area. It provides a gentle correction of the distal curve. Once the medial epicondyle flat area is exposed, the plate is introduced subperiosteally in a retrograde fashion. Later, the proximal incision, as described by Drs Livani and Belangero, is performed to identify the proximal portion of the plate. The tendon of the long head of the biceps muscle must be identified. Final attachment of the plate is performed. The most distal screw must be introduced monocortically to avoid potential damage to the ulnar nerve. At least three bicortical locking compression plate screws must be introduced distally. Postoperative physiotherapy consists of passive movements during the first 2 weeks, starting posteriorly with active mobility. To date, 31 patients have undergone surgery involving use of this technique, and no lesion of the neurovascular bundle or the ulnar nerve has been reported. There was neither superficial nor deep infection. All fractures healed except one metastatic fracture in a patient who passed away. A transient radial nerve palsy occurred that we attribute to excessive intraoperative manipulation because, as seen before, direct damage to the nerve is not possible with the technique we describe. We followed 18 patients for between 1 and 4 years, and they had good or excellent results on the Constant assessment scale and the Mayo Elbow Performance Scale. To solve the uncomfortable problem of not using an anatomic plate for this specific area, we are designing a custom plate that promises to facilitate the surgical procedure.