Ultrasound-Guided Injection of the Medial Collateral Ligament Bursa for a Degenerative Medial Meniscus Tear
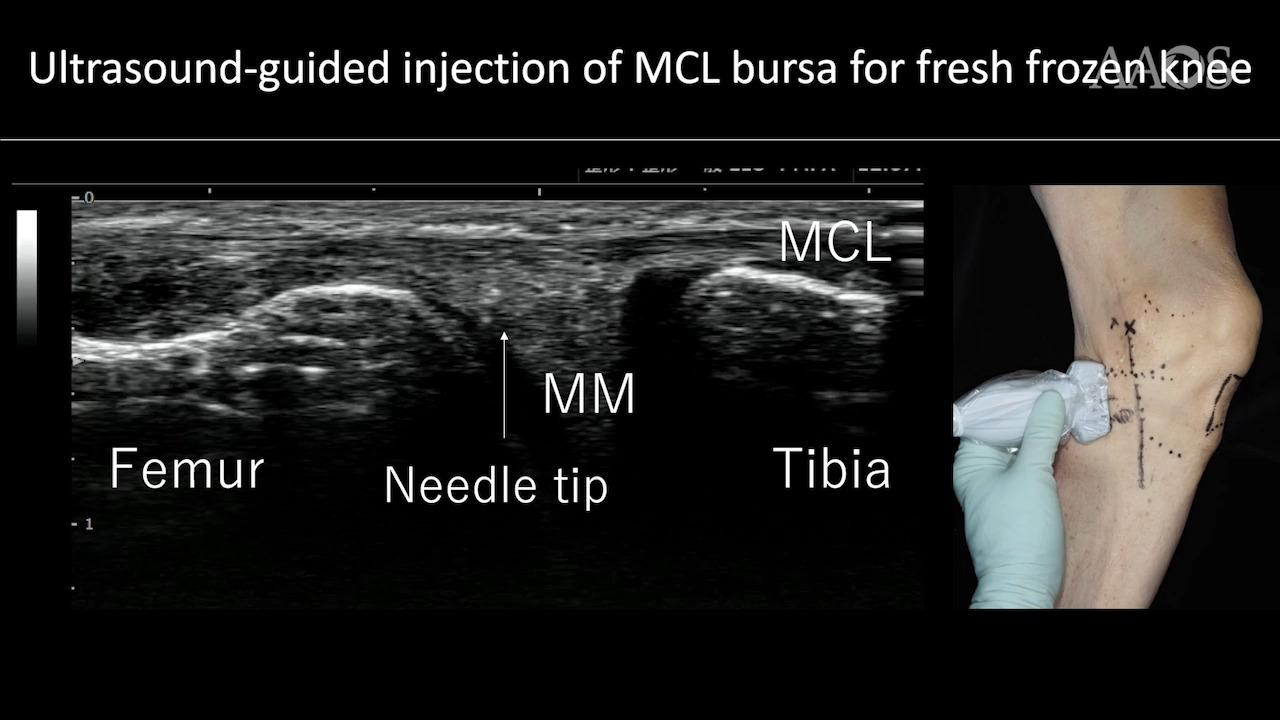
A degenerative meniscus lesion is a slowly developing lesion, typically involving a horizontal cleavage of the meniscus and generally occurring in a middle-aged or older person. Such meniscus lesions are frequent in the general population and often are incidental findings on knee MRI. In 2020, an expert consensus statement was reported in Arthroscopy. In summary, this statement noted that degenerative meniscus tears are a normal part of aging. Not all tears cause symptoms. Symptomatic patients should initially be treated nonsurgically. Repairable tears should be repaired. It is imperative to understand that degenerative meniscus lesions are extremely common. The prevalence of degenerative meniscus lesions in the general population increases with increasing age, ranging from 25% in knees of those aged 50 to 59 years to 45% in the knees of those aged 70 to 90 years. Most of these meniscus lesions do not directly cause knee symptoms, because more than 60% of tears were seen in study participants who were completely free of knee pain, aching, or stiffness. Surgery should not be proposed as a first line of treatment of degenerative meniscus lesions. If after 3 months of nonsurgical treatment the patient's pain and mechanical symptoms persist, arthroscopic surgery may be proposed. The European Society of Sports Traumatology, Knee Surgery and Arthroscopy reported in its consensus project that the main clinical challenge for the conservative management of patients with degenerative meniscal tears is the lack of evidence regarding what constitutes the best conservative treatment. From ultrasonographic findings and the anatomic location of point tenderness, we thought that one of the causes of pain in degenerative medial meniscus tears might be bursitis of the medial collateral ligament. Anatomy of MCL Bursa The MCL bursa is located between the deep and superficial MCL. De Maeseneer reported that histologically, the MCL bursa is lined by epithelial cells. The MCL bursa is located between the anterior border of the superficial MCL and the anterior part of the postero oblique ligament where the second and third layers join. The MCL bursa is very thin and cannot be injected blindly, but it can be observed with ultrasonography. Therefore, we developed ultrasound-guided injection of MCL bursa for degenerative medial meniscus tears. This injection could be a new treatment option for degenerative tears of the medial meniscus. The goal of this video is to explain the technique of ultrasound-guided injection of MCL bursa and report the clinical results. Description of the Injection Technique To perform an efficient and safe ultrasound-guided procedure of MCL bursa injection, we recommend a 25-gauge needle. We inject 1 mL of local anesthetic and 5 mg triamcinolone. A large area of skin is sterilized. The needle can be inserted at a distance of about 1 cm away from the transducer. We use the out-of-plane approach. The patient is in the supine position, with the lower limb externally rotated to correctly expose the medial side of the knee joint. We palpate the medial femoral epicondyle and place the transducer. The medial meniscus is located between femur and tibia. Moving to the flexion side, one can detect the tibial attachment of the semimembranosus direct tendon. The tibia is dented. The postero-oblique ligament begins at this line; in other words, the MCL synovial ends. On the extension side, one can see the high echoic area between the medial meniscus and the superficial MCL. This is the MCL bursa and the injection target. Anatomic Study in Cadavers We investigated three fresh frozen knees. This video shows an MCL bursa injection into a fresh frozen knee. We injected 1 mL green ink into the MCL bursa under ultrasonographic guidance. After dissection, we were able to confirm the green ink had been deposited at the MCL bursa, not intracapsularly. Injection accuracy is 100% for this technique. No anatomic specimens exhibited intrameniscal injection or demonstrated evidence of iatrogenic injury to regional structures. Results The inclusion criterion was medial knee pain of Kellgren-Lawrence grade 1 or less; 35 knees met the criteria. The average age of the participants was 51.4 years. All patients received ultrasound-guided injection for the MCL bursa. MRI was obtained within 1 week after the ultrasound-guided injection. Severity of knee pain was documented via a 0 to 10 numeric rating scale before and 1 week after the procedure. The average score on the numeric rating scale was 6.7 before the injection and 2.3 1 week after injection. The primary clinical success rating was 74.2%. Twenty-four patients reported full return to daily activities. The average number of injections was 1.7. The remaining nine patients underwent surgery: seven underwent arthroscopic surgery (repair and/or partial meniscectomy) and two underwent high tibial osteotomy owing to medial meniscus posterior root tear. Case presentation The patient was a 57-year-old woman. She was experiencing pain in the right knee without any history of trauma. The alignment was almost neutral. Her osteoarthritis was at Kellgren-Lawrence grade 1. MRI showed medial meniscus degenerative tear. Ultrasonographic findings showed medial meniscus extrusion and revascularization around the MCL bursa. This video shows the healthy side. After injection, revascularization around the MCL bursa decreased compared with preinjection. The patient's pre-injection score on the numeric rating scale was 10. There was very little pain both 2 weeks and 4 weeks after the injection. Conclusion Ultrasound-guided injection for the MCL bursa is one of the new treatments for degenerative medial meniscus tears. However, these injections were ineffective for flap tears and posterior root tears.