Primary Repair of Symptomatic Lower Leg Fascial Defect
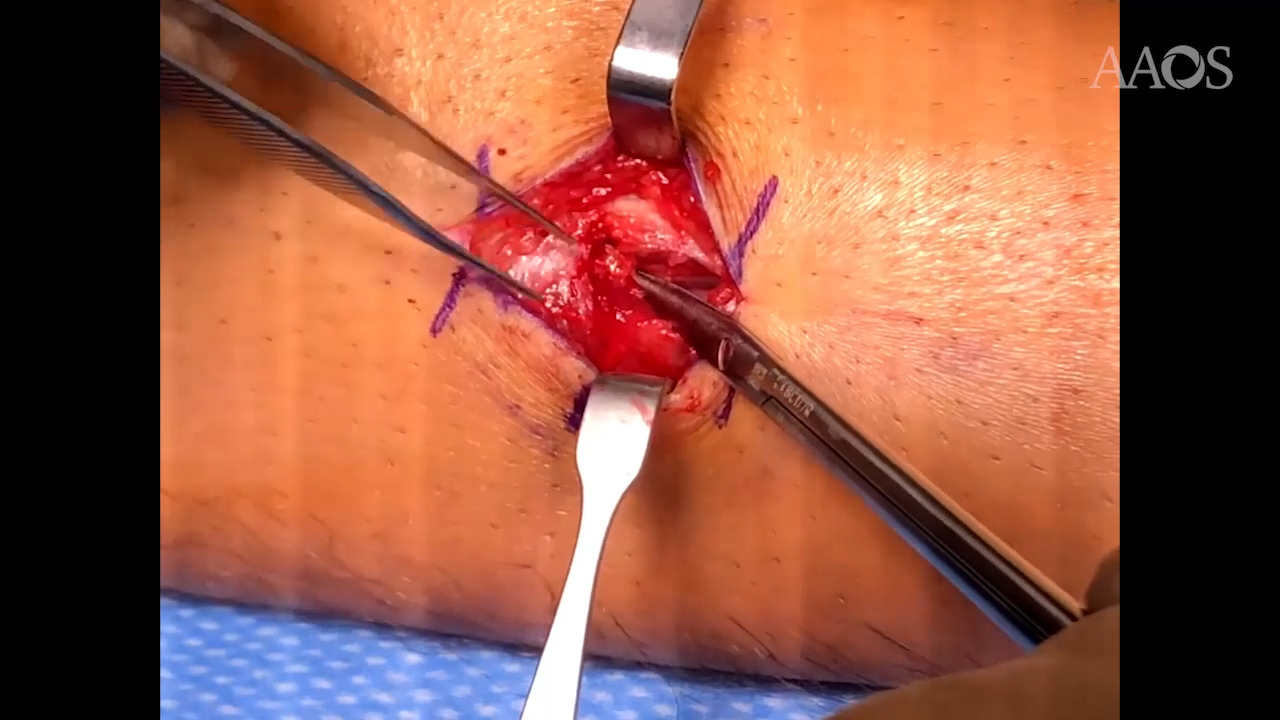
Symptomatic myofascial herniations of the extremities occur infrequently; however, they can contribute to significant pain, weakness, and neuropathy with activity. There is often a focal defect in the deep fascia through which muscle herniation occurs; this can be secondary to local trauma or congenital fascial defect. Patients often exhibit an intermittently palpable subcutaneous mass and can have neuropathic symptoms, depending on the degree of nerve involvement. Patients are initially treated with conservative modalities, whereas surgery is reserved for patients who demonstrate persistent functional limitations and neurologic symptoms. Here, we present a case of a 14-year-old boy with a defect in the lateral compartment fascia of his right lower leg that resulted in peroneus longus muscle herniation through the defect with associated superficial peroneal nerve compression, leading in turn to radiating paresthesias down the leg. Case Presentation The patient had a 3-month history of a small, intermittently present mass on the lateral aspect of the lower leg. The area enlarged with any significant activity. In particular, he had pain in the area when running and developed paresthesias down the right lateral leg and foot when playing soccer or running long distances. His symptoms resolved after about 30 minutes of inactivity. Imaging showed the muscle herniating through the fascia during passive dorsiflexion. After failure of conservative management and no abnormal masses found via MRI, a dynamic ultrasonogram was ordered. The ultrasonogram demonstrated herniation of the peroneus longus musculature through a fascia defect during muscle activation. Given these findings and the patient's desire to continue playing soccer, he and his parents elected to undergo primary closure of the lateral compartment fascia. Surgical Treatment The patient was correctly marked, a timeout was performed, a tourniquet was placed, and the leg was prepped in usual sterile fashion. A 3-cm longitudinal incision was made with a No. 15 blade scalpel directly over the area where the fascial defect was noted to be on ultrasonography. Gentle dissection was taken down to the level of the fascia with tenotomy scissors. The defect in the fascia was immediately noted. The superficial peroneal nerve was present on top of the muscle at the base of the defect exiting the area of the fascia. The peroneal nerve was gently pushed deep to the fascial defect with a freer elevator to be kept out of the way of the repair. The peroneal nerve was protected by being held underneath the freer during the entirety of the primary repair. A #2 nonabsorbable suture was then used to close the fascial defect, primarily via three figure-of-eight sutures. A nonabsorbable suture was used so that the fascia would remain closed and would not have an opportunity to re-tear. The muscle glided smoothly during passive ankle flexion and extension with no further muscular herniation after the primary repair. The wound was then irrigated with sterile normal saline and the subcutaneous tissue was closed in an interrupted fashion followed by a running subcuticular stitch for the skin. The incision healed well, with no evidence of residual herniation. Postoperative Care The patient was placed in a short leg splint to protect the primary repair after surgery. The patient was transitioned to a boot at the 2-week postoperative appointment. At 6 weeks after surgery, he reported resolution of his pain, numbness, and tingling symptoms. At this point, he was able to wean himself from use of the boot and slowly return to running; he then returned to playing soccer 10 weeks postoperatively, with no further symptoms.