Management of a Chronic Elbow Dislocation With an Internal Fixator
Management of chronic elbow dislocations is difficult and often complicated by recurrent instability, restricted range of motion, and pain. An internal fixator can be used to restore stability and facilitate early range of motion, with early results showing concentric reduction of the ulnohumeral joint and good range of motion in flexion/extension and pronation/supination.
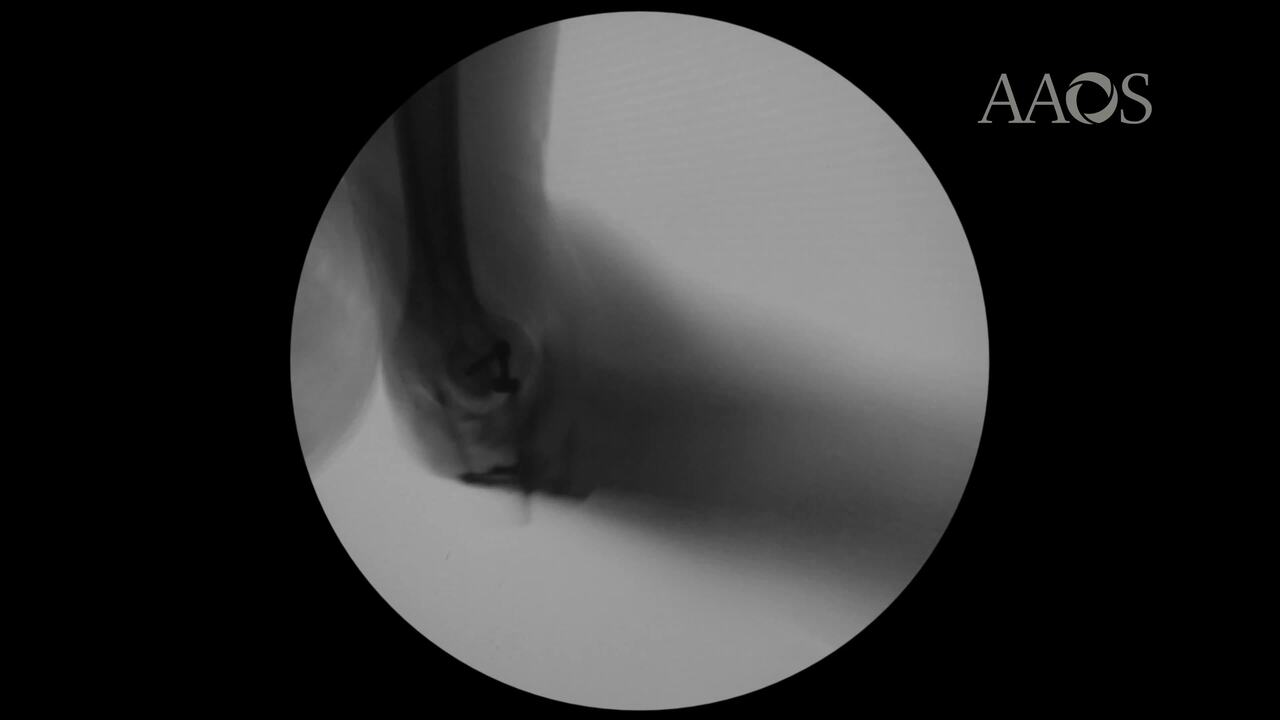
This video details the case presentation of a 72-year-old man with polytrauma who had a 6-week-old dislocation of the ulnohumeral joint and substantial heterotrophic ossification. On physical examination, the patient had extensive swelling, a 20° arc of flexion/extension, and a grossly unstable ulnohumeral joint. The patient's motor and neurologic sensory examination was intact, except for tingling in the ulnar nerve distribution.
The video reviews various treatment options, including the decision to use an internal fixator based on the priority of early restoration of range of motion. Because ulnar nerve symptoms were noted preoperatively and substantial improvements in flexion were expected postoperatively, ulnar nerve transposition was planned to avoid increased tension on the ulnar nerve.
At 6 weeks postoperatively, the patient had active range of elbow motion from 10° to 90° and a stable glenohumeral joint. At 3.5 months postoperatively, the patient had superficial wound breakdown that led to a deep infection. Hardware removal was performed, and no other complications were noted. At 6 months postoperatively, the patient was very satisfied with his improved functional status. Clinical video demonstrates a stable elbow, a 90° active arc of flexion/extension (compared with a 20° active arc of flexion/extension preoperatively), and a 90° arc of pronation/supination.
As demonstrated in this case presentation, an internal joint stabilizer facilitates concentric reduction of the ulnohumeral joint and good range of motion in flexion/extension and pronation/supination. Because of the thin subcutaneous layer around the elbow, the implant, especially the ulnar base plate, may be symptomatic; therefore, hardware removal can be planned after the soft tissues have healed.
Long-term, large patient series on internal fixation of chronic elbow dislocations are limited; therefore, the true rate of complications is difficult to determine. Recurrent instability occurs in as many as 4% of patients. Postoperative stiffness and heterotrophic ossification also have been reported but can be managed via open/arthroscopic contracture release. Ulnar neuropathy is another potential complication, especially in patients with abnormal anatomy, debridement is necessary to reduce chronic dislocations. As shown in this case presentation, ulnar nerve transposition during the index procedure is an option but may limit safe secondary arthroscopy for contracture release, if necessary. Infection also has been reported, with implant resection and antibiotic spacer placement required for management.