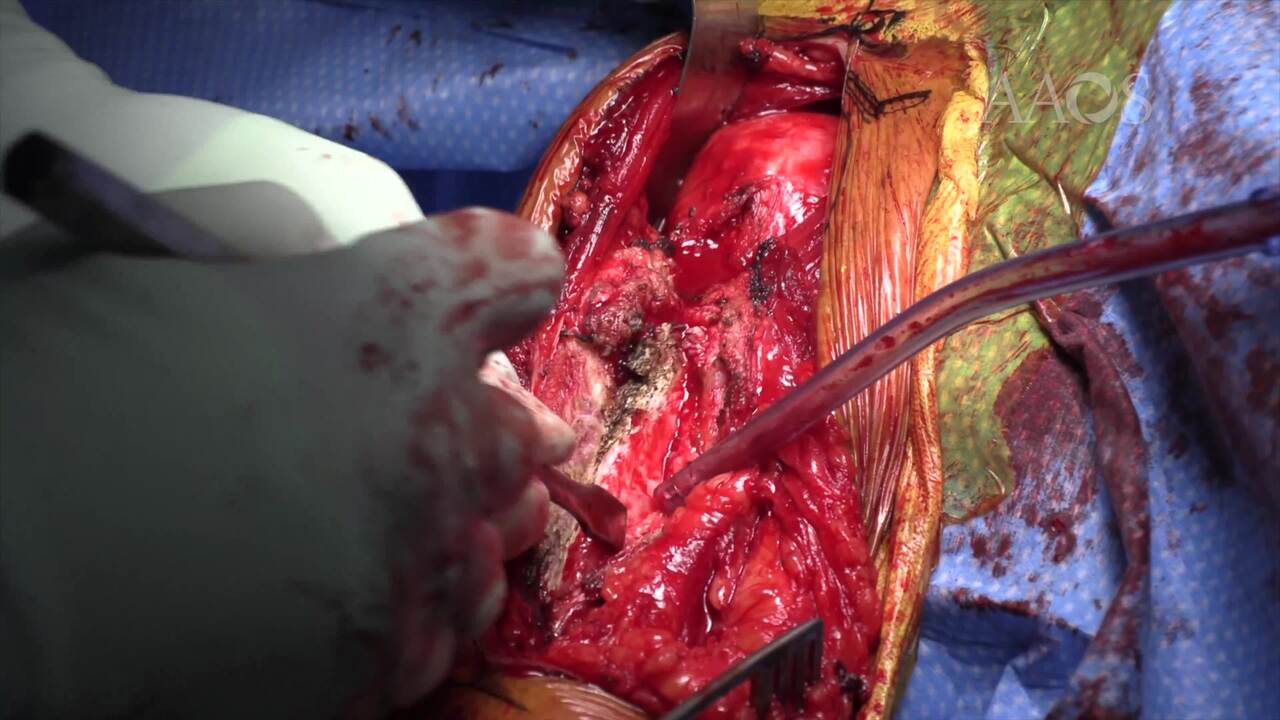
Repair of Humeral Shaft Nonunion With Plate and Screw Fixation and Iliac Crest Bone Graft
Background Humeral shaft fractures account for approximately 3% to 5% of all fractures. Approximately 30% of humeral shaft fractures occur in the proximal third of the humeral shaft. Nonunion is relatively common in patients with a humeral shaft fracture. The rate of nonunion is reported to be as high as 15%. Risk factors for nonunion include motion at the fracture site, avascularity, fracture gaps, and infection. Purpose This video and case presentation demonstrate a technique for the management of proximal third humeral shaft nonunions. The approach to the fracture, preparation of the nonunion site, nonunion fixation, and iliac crest bone harvest are discussed. The literature on and the outcomes of proximal third humeral shaft fracture nonunions also are reviewed. Methods An overview of the pathogenesis, diagnosis, and management of humeral shaft nonunions is presented, and the fixation technique is demonstrated. Particular attention is paid to nonunion preparation. A review of the literature on fixation strategies and biologic augmentation also is provided, and the outcomes of the management of humeral shaft nonunions performed by the senior author are summarized. Results The procedure was successfully performed, and the nonunion site healed. The patient was advanced through a standardized rehabilitation protocol. The patient had a pain free, functional arm and excellent overall outcomes at 1 year postoperatively. The senior author’s series of 72 patients with a humeral shaft nonunion managed via plate and screw osteosynthesis and iliac crest bone graft resulted in successful union in 98% of the patients, with a 4% rate of complications, which included one infection and one periprosthetic fracture. Conclusion Humeral shaft nonunions are relatively common; however, careful surgical management, including nonunion site preparation, compressed bony apposition, and biologic augmentation, may result in reliable outcomes. Results at 1 year postoperatively show good to excellent outcomes with this fixation technique.