A Novel Technique for Rotator Cable–Preserving Repair of Isolated Subscapularis Tears: Modified Double-Row Suture Bridge Repair
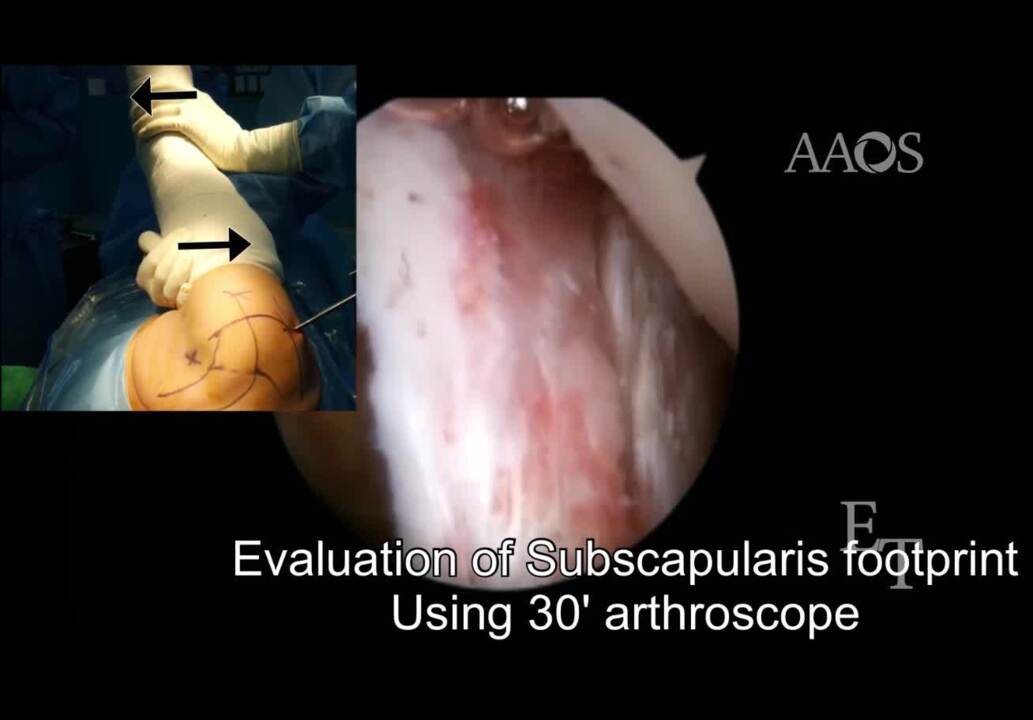
The reported prevalence of subscapularis tears varies. Approximately 10% to 30% of subscapularis tears are detected via arthroscopy. Most subscapularis tears involve the superior third of the tendon, and partial subscapularis tears associated with an anterosuperior rotator cuff tear lesion are common. Isolated, complete subscapularis tears are less common than superior rotator cuff or combined tears but are a cause of pain and functional impairment. Repair of isolated subscapularis tears account for approximately 4% of all arthroscopic rotator cuff repair procedures. Initially, open repair was used to manage subscapularis tears. However, with the development of arthroscopy, arthroscopic repair currently is mainly performed, resulting in good outcomes. Various arthroscopic repair techniques are available, including single-row, double-row, pseudo–double-row, and transosseous suture bridge techniques. Knot configuration techniques include the mattress, the Mason-Allen, the modified Revo, the U-stitch , and the lasso-loop techniques. Studies have reported that the double-row suture bridge technique is associated with a biomechanically higher ultimate load, higher stiffness, smaller elongation, and maximal contact area for tendon-to-bone healing compared with the single-row technique. The double-row technique is associated with a lower rate of re-tear and improved tendon healing. Burkart et al proposed an anatomic structure called the rotator cable and explained that it plays a biomechanical role, acting as a stress shield for the rotator crescent, which is the avascular insertion site of the supraspinatus and infraspinatus. The authors compared the rotator cable to a suspension bridge, explaining that it can protect the rotator crescent, which is susceptible to tear, by keeping load stress out of the rotator crescent. In a cadaver shoulder model study, Mesiha et al reported that tears that involve the anterior rotator cable are associated with larger tear size and are accompanied by reduced tendon stiffness and increased tendon stress. Cho et al reported larger and more complex tear patterns, more fatty degeneration, and a higher rate of re-tear in patients with tears that involved the anterior rotator cable. Denard et al discussed the relationship between rotator cable integrity and pseudoparalysis. The biceps pulley is a structure directly involved in the stability of the long head of the biceps and is located within the rotator interval between the anterior edge of the supraspinatus tendon and the superior edge of the subscapularis tendon. The biceps pulley consists of the superior glenohumeral ligament and the coracohumeral ligament. The coracohumeral ligament is divided into the medial coracohumeral ligament and the lateral coracohumeral ligament. The lateral coracohumeral ligament is anatomically connected to the anterior rotator cable. Therefore, damage to the rotator cable also may affect the bicep pulley, affecting its stability. In previous studies on subscapularis repair, the double-row suture bridge technique was performed by exposing the biceps groove for the involved rotator cable in patients with an anterosuperior rotator cuff tear. Although the double-row suture bridge technique results in superior biomechanical properties, using this technique in patient with an isolated subscapularis tear may result in injury to the anterior rotator cable and the biceps pulley. Therefore, we developed a modified double-row suture bridge technique for patients with an isolated subscapularis tear that preserves the anterior rotator cable and the bicep pulley. This technique retains the advantages of the double-row suture bridge technique, including a better biomechanical effect and footprint coverage, but preserves the anterior rotator cable and biceps pulley via a modified suture vector from the existing double-row technique. The modified double-row suture bridge technique for the management of isolated subscapularis tears involves the use of a 30&[deg] arthroscope. Indications for this technique include an isolated subscapularis tear with a preserved rotator cable and a biceps pulley structure or a tear that involves the upper two-thirds of the subscapularis (Lafosse type 1, type 2, or type 3). This technique is contraindicated in patients with an irreparable subscapularis tear. The advantages of this technique include the following: (1) it improves rotator cuff integrity and biceps stability via preservation of the rotator cable and the biceps pulley; (2) it improves fixation strength and footprint coverage to prevent re-tear; (3) it is an all intra-articular procedure; (4) it involves the use of only one familiar 30&[deg] arthroscope; (5) it involves the use of only one viewing portal; (6) it is simple and easy to perform; and (7) it is associated with a short learning curve. The disadvantages of the technique are that it can only be used to manage isolated subscapularis tears and it requires an additional anterior portal.