Hook of Hamate Excision for Symptomatic Nonunion
Case Overview
This video discusses the case presentation of a 21-year-old man with chronic hypothenar pain secondary to a left hook of hamate nonunion after a baseball injury.
Method/Technique
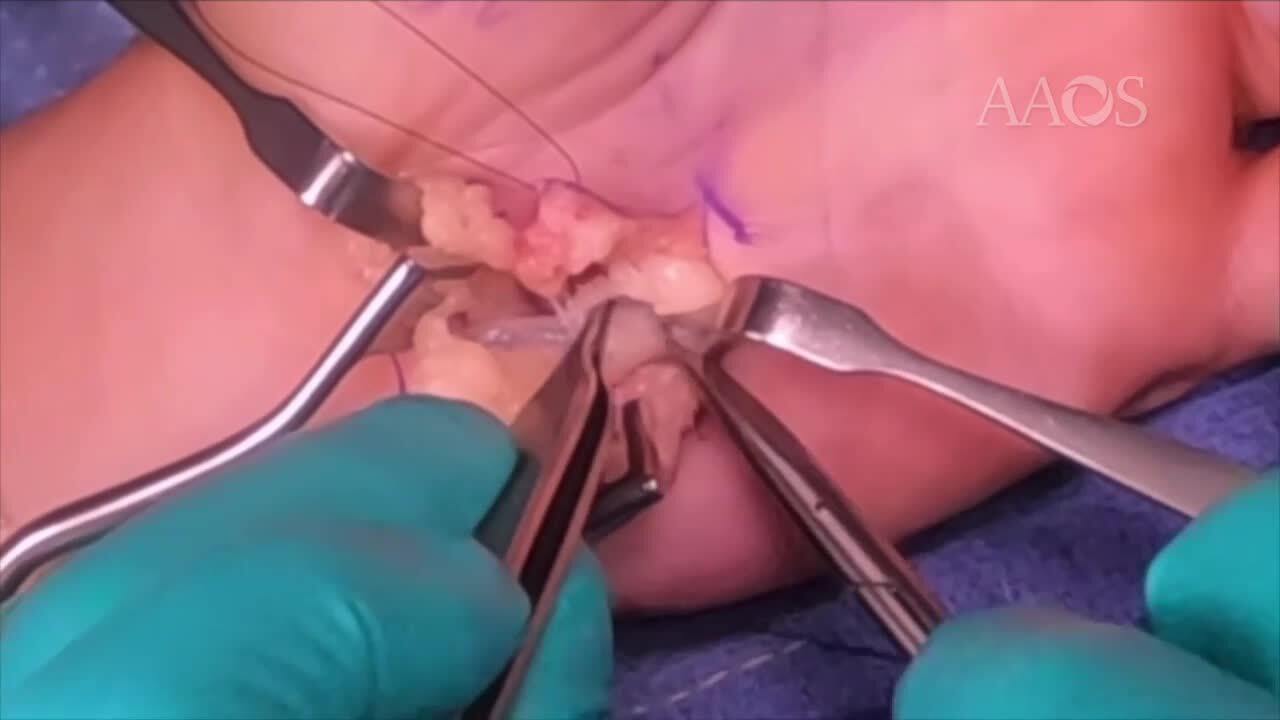
Landmarks identified prior to incision include the flexor carpi ulnaris; the pisiform; the Kaplan cardinal line; and the hook of hamate, which is one finger-breadth diagonal in the radial direction from the pisiform. Exposure is attained with the use of an ulnar sided, volar, zigzag Brunner-type incision crossing the wrist joint. The skin is incised, after which blunt scissor dissection is performed through the subcutaneous tissues to protect the ulnar nerve, ulnar artery, and small cutaneous sensory branches. The palmar carpal ligament/fascia is incised to expose the ulnar nerve/artery. The two to three transverse branches of the ulnar artery overlying the ulnar nerve are cauterized. The ulnar nerve, which is deep and ulnar to the artery, is exposed proximally and distally, including the motor branch of the ulnar nerve as it courses distally around the hook of hamate. The distal portion of the transverse carpal ligament is sharply released from its insertion on the radial aspect of the hook of hamate. A beaver blade is then used to gain access to the fibrous nonunion site to free the fracture fragment, which is removed with the use of a rongeur. An osteotome is used to smooth the fracture bed, preventing any motor branch irritation.
Results
Several retrospective studies assessing the outcomes of hook of hamate excision in athletes reported predictable pain relief, early return to play, and limited complications.
Summary
Hook of hamate excision is an excellent treatment option for patients with a symptomatic nonunion.