Subscapularis-Sparing Rotator Interval Approach for Anatomic Total Shoulder Arthroplasty
Background
A subscapularis-sparing approach for anatomic total shoulder arthroplasty (TSA) is used for patients with glenohumeral osteoarthritis who have an intact rotator cuff and sufficient bone volume.
Description
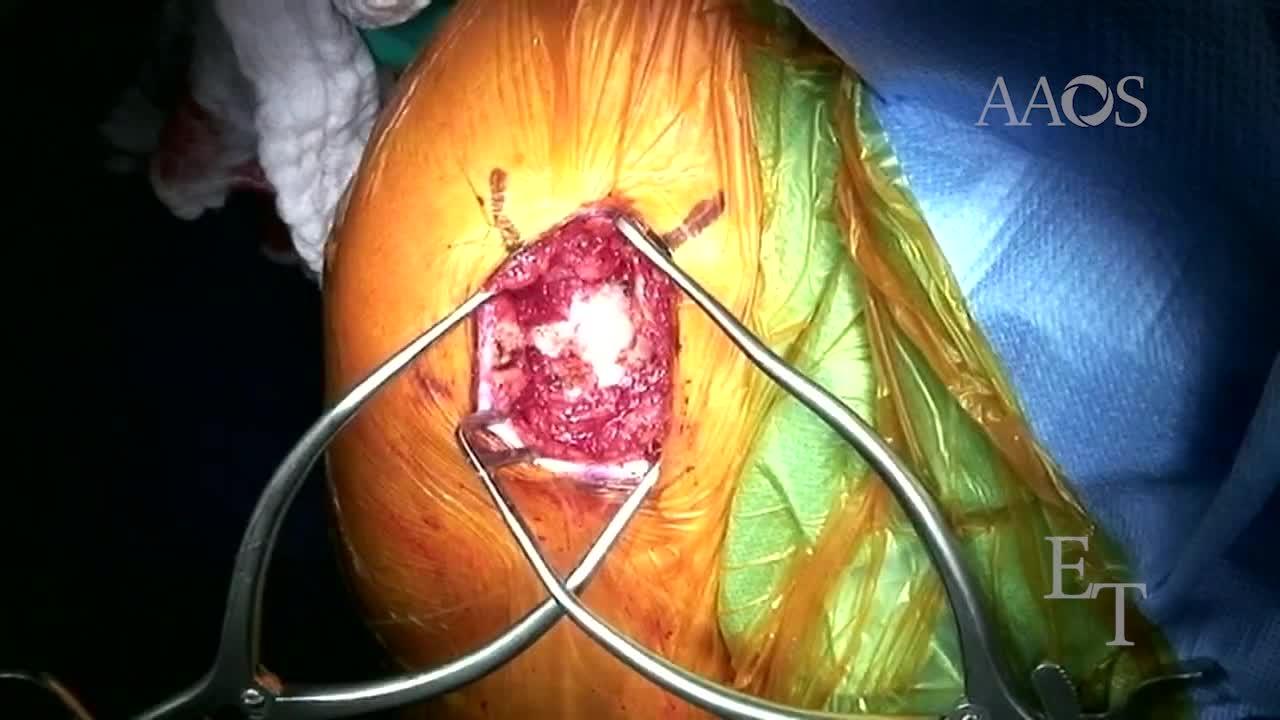
The patient is placed in the beach-chair position, and a 7- to 10-cm anterosuperior incision is made. The anterolateral deltoid raphe muscle is split, and the shoulder is externally rotated to bring the rotator interval into the field. A flap of interval tissue is incised, the biceps tendon is tenodesed, and the interval tissue is incised straight back toward the glenoid from the upper edge of the subscapularis, creating a triangular piece of tissue referred to as a trap door. Two Darrach retractors are placed to expose the humeral head. An intramedullary guide is placed, and a humeral head osteotomy is performed. The glenoid is exposed, and the glenoid component is placed after sizing, preparation, drilling, and trialing per surgical technique. The humeral head size is estimated by measuring, and the humeral stem size is selected by sequentially inserting trials. The definitive humeral stem is inserted, and the definitive humeral head is inserted after trialing. The trap door piece of tissue is sutured, the deltoid is reattached, and subcutaneous tissue and skin are sutured.
Alternatives
The traditional surgical approach for anatomic TSA involves take down and reattachment of the subscapularis tendon.
Rationale
Almost all techniques for anatomic TSA require subscapularis release via a peel, tenotomy, or osteotomy and repair on completion of TSA. Failed subscapularis healing is a devastating complication after anatomic TSA, leading to decreased function, instability, and pain. Subscapularis dysfunction after anatomic TSA occurs in one-third to two-thirds of patients with evidence of a complete tear and in as many 50% of asymptomatic patients. Sling immobilization and the avoidance of excessive passive external rotation and active internal rotation are recommended to prevent postoperative subscapularis rupture. However, postoperative motion restrictions to protect the subscapularis may lead to stiffness and negatively affect function and patient satisfaction. This video describes subscapularis-sparing anatomic TSA, which addresses three technical difficulties of anatomic TSA identified by Lafosse et al. These technical difficulties include ensuring an anatomic humeral neck cut, inadequate resection of inferior humeral neck osteophytes, and undersizing of the humeral head.