Arthroscopic Excision of Localized Pigmented Villonodular Synovitis of the Knee
Pigmented villonodular synovitis (PVNS), which also is known as a tenosynovial giant cell tumor or a giant cell tumor of the tendon sheath, is a rare proliferative disease of the synovial membrane, bursa, and tendon sheath that exists in localized and diffuse forms. PVNS was once thought to be the result of chronic inflammation or trauma-induced hemorrhage; however, recent research suggests a neoplastic origin. Localized PVNS typically is a monoarticular process, most commonly affecting the knee. Patients classically present in their thirties through fifties with a chronically swollen joint and may report a palpable mass or mechanical symptoms, such as locking. Radiographs often appear normal but may demonstrate osseous erosion from direct pressure. Localized PVNS has an almost pathognomonic appearance of a well-defined soft-tissue mass with focal hypointense areas on T1-weighted and T2-weighted MRIs. Regardless, biopsy is the preferred method for diagnosis, with histology revealing hemosiderin deposition and an abundance of mononuclear histiocyte-like cells, lymphocytes, and multinucleated giant cells. For patients with minimal symptoms, localized PVNS can be monitored via serial clinical examinations and/or MRI. Surgical excision, either open or arthroscopic, can be performed in symptomatic patients. Given its efficacy and decreased morbidity, arthroscopic excision generally is regarded as the first line treatment. Several studies have reported excellent functional outcomes in patients with PVNS who undergo arthroscopic excision, with recurrence rates equivalent to those of open excision.
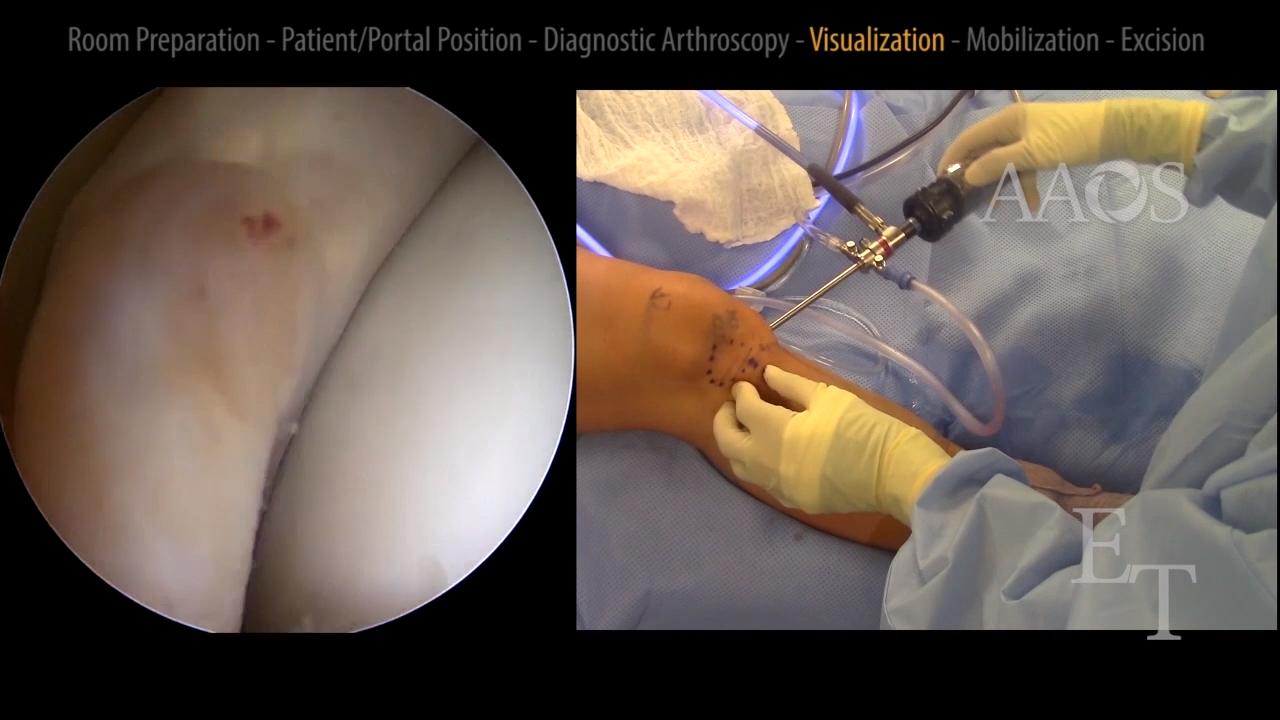
This video demonstrates arthroscopic excision of localized PVNS from the inferolateral aspect of a knee. Emphasis is placed on preoperative localization of the lesion via a physical examination and MRI to ensure the lesion and the surrounding synovium can be completely excised via arthroscopy and to determine optimal portal locations. Patient presentation, physical examination findings, imaging studies, and the postoperative rehabilitation protocol are discussed, and published clinical outcomes are briefly reviewed.