Syndesmotic Injuries: Physical Examination, Diagnosis, and Arthroscopic-Assisted Reduction
An ankle syndesmotic injury, which also is known as a high ankle sprain, may be difficult to diagnose and differentiate from a common ankle sprain. The syndesmosis is composed of static and dynamic anatomic structures working symbiotically to create a stable yet highly dynamic relationship between the tibia and the fibula. The key static stabilizer is the incisura, which is a concave groove in the distal tibia in which the fibula rotates. The syndesmotic ligamentous structures are composed of the anteroinferior tibiofibular ligament, the interosseous membrane, the posteroinferior tibiofibular ligament, and the inferior transverse ligament. Syndesmotic injury typically results from high-speed collisions or rotational injuries that cause the foot to externally rotate while in a dorsiflexed position. Because of the mechanism of injury, minimal trauma to the lateral ankle ligaments is present in patients with a high-grade syndesmotic injury. Approximately 17% of lateral ankle sprains are associated with a concurrent low- to high-grade syndesmotic injury. Diagnosis of syndesmotic injury requires several physical examination findings and radiographic findings and strong clinical suspicion. Surgeons must be able to restore anatomy and function in patients with a syndesmotic injury; however, the paucity of techniques and vague descriptions may make this difficult.
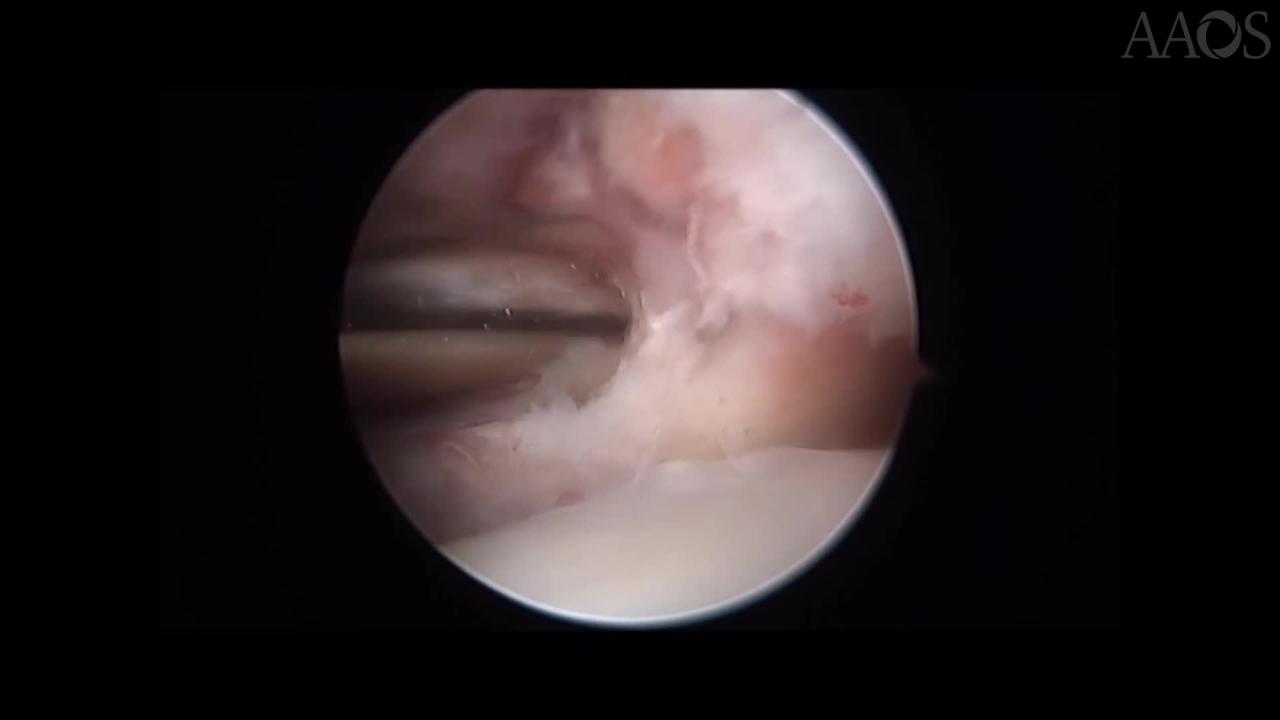
This video demonstrates the diagnostic examinations for and arthroscopic-assisted reduction in patients with a syndesmotic injury based on current evidence-based medicine. Obtaining a thorough patient history is essential because many syndesmotic injuries are missed or incorrectly diagnosed. The physical examination is performed systematically, beginning with the least painful and progressing to help with useful compliance. Standard lower extremity weight-bearing radiographs should be obtained, including views of the ankle and the tibia, to rule out fracture and evaluate joint symmetry. Stress radiographs also may be beneficial. The lead author (K.D.M.) prefers a gravity stress examination, which minimizes pain and can be reliably performed by a radiographic technician. Although plain radiography is the imaging modality most commonly used to evaluate the syndesmosis, the usefulness of radiography for the diagnosis of syndesmotic injury is limited. MRI has been reported to be 100% sensitive, 93% specific, and 96% accurate for the diagnosis of syndesmotic injury. Suture-button fixation of the distal tibiofibular joint has been increasing in popularity compared with the use of syndesmotic screws. Although both these techniques result in similar outcomes, some aspects of suture-button fixation, including the absence of implant breakage and the decreased need for implant removal, are desirable. Cadaver model studies have demonstrated that suture-button fixation allows for correct clamp malreduction. Although good clinical outcomes have been achieved in patients who undergo suture-button fixation, inadequate stability has been reported. Studies have suggested that suture-button fixation with suture-tape augmentation of the anteroinferior tibiofibular ligament may be appropriate for the management of syndesmotic injuries in patients with lateral ankle instability. Immediately postoperatively, patients are placed in an U and L splint and are instructed to remain non-weight-bearing for 10 to 14 days postoperatively. At 2 weeks postoperatively, range of motion exercises, including ABCs and recumbent biking, are initiated. At 4 weeks postoperatively, formal physical therapy and 25% weight-bearing are initiated, increasing weight-bearing by 25% per week as tolerated.